

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Similar a Psoriasis
Similar a Psoriasis (20)
Más de Vineetha Menon
Más de Vineetha Menon (8)
Último
Último (20)
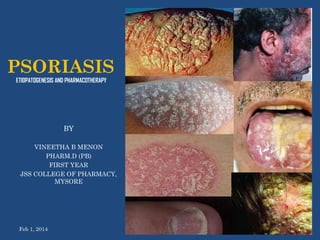
Psoriasis
- 1. PSORIASIS ETIOPATOGENESIS AND PHARMACOTHERAPY BY VINEETHA B MENON PHARM.D (PB) FIRST YEAR JSS COLLEGE OF PHARMACY, MYSORE Feb 1, 2014 1
- 2. CONTENTS INTRODUCTION EPIDEMIOLOGY AETIOLOGY PATHOGENESIS DIAGNOSIS CLINICAL FEATURES TREATMENT Feb 1, 2014 2
- 3. INTRODUCTION • Psoriasis is a chronic inflammatory condition that may affect the skin and joints Feb 1, 2014 3
- 4. • EPIDEMIOLOGY Feb 1, 2014 4
- 5. EPIDEMIOLOGY • Psoriasis affects both sexes equally • Can occur at any age, although it most commonly appears for the first time between the ages of 15 and 25 years Feb 1, 2014 5
- 6. • AETIOLOGY Feb 1, 2014 6
- 8. • PATHOGENESIS Feb 1, 2014 8
- 9. PATHOGENESIS •Many changes occur in the skin •Epidermis – Acanthosis, Parakeratosis •Dermis – capillaries are dilated, twisted, closer to the surface of the skin Feb 1, 2014 9
- 10. • Large number of inflammatory cells are present in all layers of the skingranulocytes are predominant and form micro-abscessess in the epidermis • Langerhan cells and lymphocytes are also increased • Main abnormality is epidermal cell turn over Feb 1, 2014 the increased 10
- 11. Two hypothesis: 1. Hyperproliferation may be due to immunological response. Cytokines released by lymphocytes and langerhan cells may further stimulate the inflammatory cells which cause epidermal cell turn over at an increased rate Feb 1, 2014 11
- 12. 2. Epithelial cells themselves produce cytokines which promote proliferation of epithelial cells and attract lymphocytes Feb 1, 2014 12
- 13. • DIAGNOSIS Feb 1, 2014 13
- 14. DIAGNOSIS • A diagnosis of psoriasis is usually based on the appearance of the skin • There are no special blood tests or diagnostic procedures • Skin biopsy, may be needed to rule out other disorders and to confirm the diagnosis • Skin from a biopsy will show clubbed rete pegs, if positive for psoriasis • Another sign of psoriasis is that when the plaques are scraped, one can see pinpoint bleeding from the skin below Feb 1, 2014 14
- 15. Rete pegs are the epithelial extensions that project into the underlying connective tissue Feb 1, 2014 15
- 16. • CLINICAL FEATURES Feb 1, 2014 16
- 17. CLINICAL FEATURES • Typical psoriatic lesion is red, scaly, sharply demarcated plaque Feb 1, 2014 17
- 18. • It can be on any size and can affect any part of the body Feb 1, 2014 18
- 19. • The scales are silvery and easily scraped off revealing tiny bleed points • Psoriasis is not typically itchy, but it can cause itching when severely inflammed and rapidly spreading to the palms and soles Feb 1, 2014 19
- 20. • Different patterns of psoriasis are: 1. 2. 3. 4. 5. 6. 7. Guttate psoriasis Chronic plaque psoriasis Psoriasis of scalp Psoriasis of nails Psoriasis of palms and soles Flexural psoriasis Erythrodermic and generalized pustular psoriasis 8. Psoriatic arthropathy Feb 1, 2014 20
- 21. GUTTATE PSORIASIS Multiple small plaques are seen all over the body Mainly seen in children after streptococcal sore throat Self limiting after a few weeks Feb 1, 2014 21
- 22. CHRONIC PLAQUE PSORIASIS Medium and large plaques occur on the limb and trunk Very persistent Feb 1, 2014 22
- 23. PSORIASIS OF THE SCALP May occur as demarcated plaques or may involve the entire scalp extending to the hairline Scales are white, thick and chalky Hair loss will occur if the scalp is thickly scaled Recover if the scales are cleared and kept under control Feb 1, 2014 23
- 24. PSORIASIS OF THE NAILS Pitting, onycholysis and hyperkeratosis under the nail Very resistant Feb 1, 2014 24
- 25. PSORIASIS OF THE PALMS AN SOLES Sharp demarcation of the involved areas Affected areas are inflammed and scaly and may contain sterile pustules of large pin head size. These pustules dry up and form brown macules Affected skin becomes hyperatotic and fissuring Secondary infection with itching and pain are common Feb 1, 2014 25
- 26. FLEXURAL PSORIASIS Psoriasis occurs in the axillae, submammary areas, groin and genitalia Demarcation is present, but the affected areas are glazy rather than scaly and is bright red in color Feb 1, 2014 26
- 27. ERYTHRODERMIC AND GENERALIZED PUSTULAR PSORIASIS Severe and life threatening condition Uncommon Whole skin surface is involved and highly inflammed and the patient is sick Pustules are sterile and coalesce to form sheets of pus Feb 1, 2014 27
- 28. PSORIATIC ARTHROPATHY Occurs in 5% of the patients with psoriasis Similar to RA, but RF is negative Different patterns: 1. 2. 3. Feb 1, 2014 Distal Arthritis Large Joint Involvement Spodilitis/ Sacroiliitis 28
- 29. • TREATMENT Feb 1, 2014 29
- 30. TREATMENT Aimed at controlling the current attack and not curing, and does not influence future progress of the disease TOPICAL THERAPY 1. Emolients 2. Topical Steroids 3. Dithranol 4. Coal Tar 5. Salicylic Acid 6. Vitamin D Analogues 7. UVB Feb 1, 2014 SYSTEMIC THERAPY 1. PUVA 2. Cytotoxic Drugs 3. Immunosuppressant Drugs 4. Acitretin 5. Photodynamic Therapy 6. Systemic Steroids 30
- 31. TOPICAL THERAPY 1. EMOLIENTS • Used alone in very mild cases • Used along with other therapies for moderate to severe disease Feb 1, 2014 31
- 32. 2. TOPICAL STEROIDS • Most useful for acutely inflammed psoriasis • Mild steroids are used on face and flexures • Potent steroids are used on hands and feet; in combination with Clioquinol or Salicylic acid • Aq. and alcoholic solutions cause stinging and burning, thus usually ointments, creams and mousse are prefered • Use of potent steroids on large areas of psoriasis may cause rebound flare when discontinued Feb 1, 2014 32
- 33. Feb 1, 2014 33
- 34. 4. COAL TAR • Used in combination with emolients, topical steroids, and salicylic acid • Used for guttate psoriasis, psoriasis of the scalp, and localized pustular psoriasis of the palms and soles • Efficiency of coal tar is enhanced when used with UVB Feb 1, 2014 34
- 35. 5. SALICYLIC ACID • Useful to remove the scales • Used in preparation for other treatment Feb 1, 2014 35
- 36. 6. VITAMIN D ANALOGUES • Efficacy of topical vit D analogues is enhanced when used in combination with topical steroids and UVB • Calciptriol & Tacalcitol • Calciptriol is more effective than coal tar and dithranol. It cannot be used on face. • Tacalcitol is used for once daily treatment of chronic plaque psoriasis. It can be used on the face Feb 1, 2014 36
- 37. 7. UVB • Short wavelength ultraviolet light is used in combination with coal tar or dithranol • Narrow band UVB is more effective Feb 1, 2014 37
- 38. SYSTEMIC THERAPY 1. PUVA • Used for the treatment of moderate to severe chronic plaque psoriasis • PSORALENS: drugs that are activated by UVA (320400nm), to interfere with the DNA synthesis and reduce the epidermal cell turn over • Eg: 5-methoxy psoralen & 8-methoxy psoralen • Can be administered orally or it can be applied topically Feb 1, 2014 38
- 39. The time of exposure is calculated based upon the previous light testing and the time interval is increased if tolerated by the patient as the treatment progresses Treatment is given twice weekly for 6 weeks Unless the disease is severe, maintenance dose is avoided to minimize the long term side effects Adverse effects: Nausea, pruritis, dry skin, aging of the skin, melanoma and non-melanoma skin cancer Feb 1, 2014 39
- 40. 2. CYTOTOXIC DRUGS • Methotrexate & hydroxycarbamide • METHOTREXATE • Most effective in the treatment of psoriatic arthritis • Test dose- 2.5 mg • Then 30 mg weekly • Side effects: nausea, fatigue, GI bleeding Feb 1, 2014 40
- 41. • HYDROXYCARBAMIDE • It should be used continuously as relapse will occur when the drug is stopped • Causes bone marrow depression Feb 1, 2014 41
- 42. 3. IMMUNOSUPPRESSANT DRUGS • CICLOSPORIN • Severe psoriasis • Dose is 2-5 mg/kg/day • Relapse may occur when the drug is stopped but intermittent therapy is preferred to maintenance therapy • Avoid sun over exposure, PUVA & UVB therapy Feb 1, 2014 42
- 43. 4. ACITRETIN • Used for severe resistant psoriasis, acute pustular psoriasis, and palmoplantar psoriasis • Has teratogenic effect • Re-PUVA therapy: acitretin + PUVA • It causes bone maturation abnormality, LFT and serum lipid levels • Causes dry skin and hair loss Feb 1, 2014 43
- 44. 5. PHOTODYNAMIC THERAPY • 5-aminolaevullinic acid (ALA) causes local accumulation of proto porphyrin 9 which is activated by irradiation with visible light and causes tissue destruction • Used for localized plaque psoriasis • Causes burning sensation at the site of treatment Feb 1, 2014 44
- 45. 6. SYSTEMIC STEROIDS • Not commonly used • May be used for the management of life threatening erythroderma • Systemic steroids or their withdrawal may itself provoke acute generalised pustular psoriasis Feb 1, 2014 45
- 46. Feb 1, 2014 46