

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Manyasthambha
Similar a Manyasthambha (20)
Más de Ayurmitra Dr.KSR Prasad
Más de Ayurmitra Dr.KSR Prasad (20)
Último
Último (20)
Manyasthambha
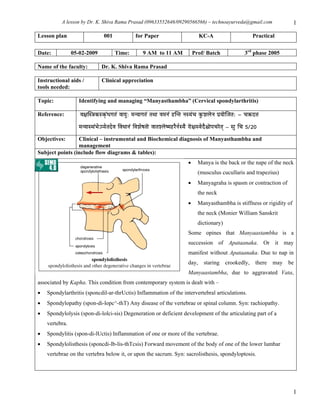
- 1. A lesson by Dr. K. Shiva Rama Prasad (09633552646/09290566566) – technoayurveda@gmail.com 1 Lesson plan 001 for Paper KC-A Practical Date: 05-02-2009 Time: 9 AM to 11 AM Prof/ Batch 3rd phase 2005 Name of the faculty: Dr. K. Shiva Rama Prasad Instructional aids / Clinical appreciation tools needed: Topic: Identifying and managing “Manyasthambha” (Cervical spondylarthritis) Reference: uɤÉÎx§ÉMüxMçüÇkÉaÉiÉÇ uÉÉrÉÑ: qÉlrÉÉaÉiÉÇ iÉjÉÉ uÉqÉlÉÇ WûÎliÉ lÉxrÉÇcÉ MÑüzÉsÉãlÉ mÉërÉÉãÎeÉiÉ: - cÉ¢üS¨É qÉlrÉÉxjÉÇpÉåÅmrÉåiÉSåuÉ ÌuÉkÉÉlÉÇ ÌuÉzÉåwÉiÉÉã uÉÉiÉzsÉãwqÉWûUælÉïxrÉæ UÉã¤ÉxuÉåSæ¶ÉÉãmÉcÉUãiÉç – xÉÑ ÍcÉ 5/20 Objectives: Clinical – instrumental and Biochemical diagnosis of Manyasthambha and management Subject points (include flow diagrams & tables): • Manya is the back or the nape of the neck (musculus cucullaris and trapezius) • Manyagraha is spasm or contraction of the neck • Manyasthambha is stiffness or rigidity of the neck (Monier William Sanskrit dictionary) Some opines that Manyaastambha is a succession of Apataanaka. Or it may manifest without Apataanaka. Due to nap in day, staring crookedly, there may be Manyaastambha, due to aggravated Vata, associated by Kapha. This condition from contemporary system is dealt with – • Spondylarthritis (sponcdil-ar-thrUctis) Inflammation of the intervertebral articulations. • Spondylopathy (spon-di-lopc^-thT) Any disease of the vertebrae or spinal column. Syn: rachiopathy. • Spondylolysis (spon-di-lolci-sis) Degeneration or deficient development of the articulating part of a vertebra. • Spondylitis (spon-di-lUctis) Inflammation of one or more of the vertebrae. • Spondylolisthesis (sponcdi-lb-lis-thTcsis) Forward movement of the body of one of the lower lumbar vertebrae on the vertebra below it, or upon the sacrum. Syn: sacrolisthesis, spondyloptosis. 1
- 2. A lesson by Dr. K. Shiva Rama Prasad (09633552646/09290566566) – technoayurveda@gmail.com 2 Clinical diagnosis: Most Common Causes of Neck Pain Etiology Typical history Key physical Key lab findings examination findings Spondylosis Dull neck ache Tender to Radiograph (x-ray) shows palpation midline degenerative changes that can Older age-group Decreased active include narrowing of disc space, Occipital headache and passive sclerosis of posterior elements, and ± radicular ROMs osteophytes symptoms Cervical disc Sharp neck pain Decreased active MRI shows disc protrusion or herniation ROM extrusion into spinal canal Burning or tingling Reduced deep in upper extremities tendon reflexes Pain with neck Decreased motion strength in upper extremities Upper extremity Positive weakness Spurling's test Cervical Intermittent dull Normal ROM X-ray is normal or shows loss of strain/sprain neck pain lordosis ± Occupational Loss of lordosis Consider computed tomography to related (postural) rule out bony injury in trauma ± Trauma history Palpable (motor vehicle tightness, accident, fall) ropiness Muscle spasm Occasional acute edema Muscle spasms Fibromyalgia Diffuse axial Normal passive No laboratory test to confirm skeletal pain ROM Sleep disturbance Trigger points Fatigue Inflammatory Dull ache Decreased active RA: increased rheumatoid factor arthritis such as and passive and erythrocyte sedimentation rate RA or AS ROMs Morning stiffness >1 Other joint AS: positive HLA B27 h inflammation Other joint involvement Referred pain Symptoms from Normal ROM of X-ray of other sites ECG, MRI other sites (e.g., neck potentially helpful chest pain, shoulder Physical examination findings at other sites (e.g., pain) shoulder strength loss, chest rales) ROM, range of motion; MRI, magnetic resonance imaging; RA, rheumatoid arthritis; AS, ankylosing spondylitis. Special Physical Examination Tests of Cervical Spine 2
- 3. A lesson by Dr. K. Shiva Rama Prasad (09633552646/09290566566) – technoayurveda@gmail.com 3 Test Evaluation for How performed Positive test Spurling's Nerve root Head in mild extension and flexion Pain in dermatomal test compression (disc toward side of radicular symptoms pattern on affected herniation) side Distraction Nerve root Head lifted axially with one hand Pain relief with test compression (disc under chin and other hand around lifting head herniation) occiput Adson's Thoracic outlet Extend patient's symptomatic Loss of pulse in maneuvers syndrome shoulder while patient rotates neck affected extremity toward affected side. Pulse is checked during deep inspiration Lhermitte's Spinal canal Patient sitting with legs extended; Shock like sensation sign narrowing (spinal ask patient to flex neck forward into lower back stenosis), multiple and/or extremities sclerosis Differential Diagnosis of Neck Pain Musculoskeletal Neurologic Infectious Neoplastic Referred Cervical strain or sprain Thoracic outlet Diskitis Spinal cord Rotator cuff syndrome tumor tendinopathy Disc herniation Peripheral Osteomyelitis Primary neck Myocardial neuropathy neoplasm ischemia Degenerative disc disease Myelopathy Meningitis Malignant Pneumonia neoplasm Inflammatory arthritis Radiculopathy Cervical lymphadenitis (rheumatoid, ankylosing spondylitis) Cervical fracture Whiplash Cervical instability Diffuse idiopathic skeletal hyperostosis Cervical stenosis Torticollis Fibromyalgia • Taylor's 10-Minute Diagnosis Manual: Symptoms and Signs in the Time-Limited Encounter, 2nded ICD-9CM CODES 722.4 Degenerative intervertebral cervical disk 722.71 Degenerative cervical disk with myelopathy Instrumental diagnosis - Computed tomography of body (Spine), Diagnostic Magnetic resonance imaging, Diagnostic Radiography (Cervical disks of spine), Diagnostic Bio-chemical Diagnosis – Creatine is synthesized in the liver, taken up by muscle cells to store energy as creatine phosphate. 3
- 4. A lesson by Dr. K. Shiva Rama Prasad (09633552646/09290566566) – technoayurveda@gmail.com 4 Creatinine is formed by hydrolysis of creatine and phosphocreatine in muscle and by ingestion of meat. When ever the only muscular involvement noted with the variances in S. Creatine and creatinine. Bone formation markers of osteoblast activity: Bone-specific alkaline phosphatase, osteocalcin, procollagen type I Bone resorption markers of osteoclast activity: Tartrate-resistant acid phosphatase (TRAP), hydroxyproline, pyridinoline, deoxypyridinoline, N-telopeptide, C-telopeptide, urine calcium - Because of diurnal rhythm, specimens should be collected at same time of day (preferably AM) Acid Phosphatase, Tartrate-Resistant (TRAP), Serum Synthesized by osteoclasts in contrast to prostatic acid phosphatase that is tartrate sensitive; also found in Kupfer cells and macrophages, thus much of males with BPH are susceptible for C.S. Use: Marker of bone resorption Alkaline Phosphatase (ALP), Bone-Specific (TRAP), Serum Synthesized by osteoblasts; is involved in calcification of bone matrix. Only ~80% of total ALP is destroyed by heating along with some nonbone-specific ALP. Use: Marker of bone formation Increased In: Paget disease; may be more sensitive than total ALP, especially when activity is low Primary hyperparathyroidism, Osteomalacia, Osteoporosis and Pregnancy • Serum Calcium, Osteocalcin (Cytosolic calcium-binding protein), etc are also bone specific chemical tests required according to situation. (Jacques Wallach M.D., Interpretation of Diagnostic Tests, 8th Edition, Lippincott, New York, P.349) • In Ayurveda it is told by Chakradatta as the condition of stiffened back at four levels as – Vaksha (thoracic) – Trika (lumbo-sacral)– Skandha (low cervical) – Manaya (high cervical); a four level vertebral diseases referred to Spondylolysis as nosology of cervical pathology. He further hints to have Kapha association and treat in conceptual with Vamana and Nasya discriminatively used by the physician. If Vamana is administered in Manyasthambha, the exertion may not be allowed by the patient and may the pain aggravate. The Vamana is administered when the physician observes the symptoms such as – sthaimitya, Sheeta, supta, sopha (inflammatory edema), gourava and snehakathinya (soft lumps). • Where in Susruta, Vata Kapha hara Dravya Nasya is administered for the Dosha elimination and externally Rooksha Sweda is offered. It looks as the Nasya (Mahamashadi Taila – Avartita) – administered to regulate the neural involved pathology of spinal level, as said lÉÉxÉÉÌWû ÍzÉUxÉÉå ²ÉUqÉç. Secondly external mediated management through – Rooksha Sweda offers the local blood supply 4
- 5. A lesson by Dr. K. Shiva Rama Prasad (09633552646/09290566566) – technoayurveda@gmail.com 5 improvement and relieves the neural conductive blocks. The dilation of bone regulates inter vertebral disk space and places to normal with soft regulative spinal massage. • Prescription of the medicaments also on the same grounds – as Kapha Vata shamaka – and vedana sthapaka. To relieve pain we commonly consider the Dashamoola, Rasna etc in Kashaya form along with guggulu enhances the effect. Abha, Nirgundi, Eranda are the single drugs used here. • Yogaraja gugulu or Trayodashanga guggulu with Maharasnadi kwatha or Rasnaspataka kwatha daily morning at Vata – Kapha sandhikala • Vatagajankusha ras tab 250 to 500mg daily twice with Dashamoolarista after meals • Mridu Abhyaga with Prabhanjana vimardana Taila / kuzumpu or Dhanwantaram Taila followed by salvana Upanaha Experimental / Practice examining cervical area for the tests told and routine Practice module Practice how to prepare “Salvana Upanaha” Assignment: Look for the combination of Vatagajankush ras and Trayodashanga guggulu for its applicability in Manyasthambha Essay • Define Manyasthambha and discuss the Nidana and Chikitsa in detail Short • Write a brief note on Manyasthambha with its management Model questions Mini • Manyasthambha Chikitsa sutra • Name the Panchakarma in Manyasthambha Fill in the • Dosha predominance in Manyasthambha is – blanks • The Sweda done in Manyasthambha is – • Multiple choice • A 55-year-old man is evaluated for weakness. Over the past few months he has noted slowly progressive weakness and cramping of his left leg. Lately he has also had some trouble swallowing food. He is awake and alert. Findings on the neurologic examination are normal except for marked atrophy with fasciculations in the muscles of both legs, hyperactive reflexes in the upper and lower extremities, a diminished gag reflex, and a positive extensor plantar response. Which of the following represents the most likely diagnosis? (A) Cervical spondylosis (B) Guillain-Barre´ syndrome (C) Lambert-Eaton syndrome (D) Vitamin B deficiency 12 (E) Amyotrophic lateral sclerosis 5
- 6. A lesson by Dr. K. Shiva Rama Prasad (09633552646/09290566566) – technoayurveda@gmail.com 6 The answer is E. Amyotrophic lateral sclerosis (ALS) is an untreatable disease that results in the progressive loss of upper and lower motor neuron function. Other components of the nervous system remain intact, including the neurons required for ocular motility. Limb weakness and cramping is the first symptom, followed by muscular atrophy, fasciculations, and loss of function of the cranial nerve musculature. Early in the disease, upper-tract signs may predominate, resulting in spasticity. Pneumonia resulting from failure of clearance of secretions is usually the terminal event. Treatable causes of motor neuron diseases such as cervical spondylosis (no bulbar involvement) and lead poisoning should be excluded whenever the diagnosis of ALS is considered. Guillain-Barre´ syndrome produces an ascending, rapidly developing paralysis. Vitamin B deficiency should lead to abnormalities in posterior column function. Lambert-Eaton syndrome is a paraneoplastic neuromuscular disorder that does not feature upper-tract signs. • Chronically progressive spinal cord disease with sensory and motor signs evolving over years may be due to (A) Kennedy’s disease (B) multiple sclerosis (C) Tay-Sach’s disease (D) lumbar disk disease (E) amyotrophic lateral sclerosis The answer is B. Several disorders produce chronic progressive spinal cord disease with sensory and motor involvement. Syndromes of spinocerebellar degeneration may involve the motor and sensory spinal cord systems in addition to causing ataxia. Multiple sclerosis usually causes a relapsing illness but can cause a progressive, usually cervical myelopathy in elderly women. Cervical spondylosis, or bony compression of the cervical cord by osteophytic bars, is another common cause of myelopathy in the elderly. Lumbar disk compression of the cauda equina, which is made up of peripheral nerves, does not cause spinal cord signs. Amyotrophic lateral sclerosis is a disease of spinal cord motor neurons and corticospinal tracts but has no sensory signs. Kennedy’s disease is an x-linked spinobulbar muscular atrophy in which there is progressive weakness and wasting of the limb and bulbar muscles. Adult Tay-Sach’s disease is a very slowly progressive disarthria with radiographically evident cerebullar atrophy. 6