ENDOTRACHEAL TUBE INTUBATION II Parts II Details II Clinical Discussion
•
153 likes•65,608 views

What is endotracheal intubation? Endotracheal intubation is a procedure by which a tube is inserted through the mouth down into the trachea (the large airway from the mouth to the lungs). Before surgery, this is often done under deep sedation. In emergency situations, the patient is often unconscious at the time of this procedure. For detailed information plz watch the slides till end....... And plz like, share and comment and follow......
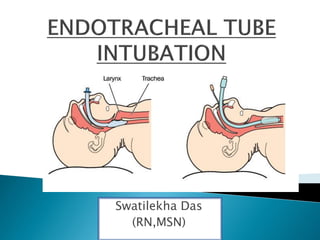
![The patient in the ICU often requires
mechanical assistance to maintain airway
patency. Inserting a tube into the trachea,
bypassing upper airway and laryngeal
structures, creates an artificial airway. The tube
is placed into the trachea via the mouth or nose
past the larynx (endotracheal [ET] intubation) or
through a stoma in the neck (tracheostomy). ET
intubation is more common in ICU patients. It
can be performed quickly and safely at the
bedside.](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Recommended
More Related Content
What's hot
What's hot (20)
Similar to ENDOTRACHEAL TUBE INTUBATION II Parts II Details II Clinical Discussion
Similar to ENDOTRACHEAL TUBE INTUBATION II Parts II Details II Clinical Discussion (20)
More from Swatilekha Das
More from Swatilekha Das (20)
Recently uploaded
Recently uploaded (20)
ENDOTRACHEAL TUBE INTUBATION II Parts II Details II Clinical Discussion
- 2. The patient in the ICU often requires mechanical assistance to maintain airway patency. Inserting a tube into the trachea, bypassing upper airway and laryngeal structures, creates an artificial airway. The tube is placed into the trachea via the mouth or nose past the larynx (endotracheal [ET] intubation) or through a stoma in the neck (tracheostomy). ET intubation is more common in ICU patients. It can be performed quickly and safely at the bedside.
- 3. Endotracheal intubation involves passing an endotracheal tube through mouth or nose into the trachea. Intubation provides a patent airway when the patient is having respiratory distress that cannot be treated with simpler methods. It is the method of choice in emergency care. Endotracheal intubation is a means of providing an airway for patients who cannot maintain an adequate airway on their own, for patients needing mechanical ventilation and for suctioning secretions from the pulmonary tree.
- 6. An endotracheal tube : provides a passage for gases to flow between a patients lungs and an anaesthesia breathing system . allows one to provide positive pressure ventilation. protects the lung from contamination from gastric contents and nasopharyngeal matter such as blood.
- 7. Indications for ET intubation include : Upper airway obstruction (e.g. secondary to burn, tumor, bleeding) Apnea High risk of aspiration Ineffective clearance of secretions Respiratory distress Respiratory arrest. Cardiac arrest
- 8. The following are only relative contraindications to tracheal intubation: Severe airway trauma or obstruction that does not permit safe passage of an endotracheal tube. Emergency cricothyrotomy is indicated in such cases. Cervical spine injury, in which the need for complete immobilization of the cervical spine makes endotracheal intubation difficult. Mallampati Classification of class III / IV or other determination of potential difficult airway.
- 9. Endotracheal tube for proper size Average female size, 7.5-8.0 mm Average male sixe, 8.5-9.0 mm Stylet (metal wire) Larynscope and blade Straight blade (Miller) Curved blade (Macintosh) Suction Tonsil tip (Yankauer) Suction kit
- 10. Syringe to inflate balloon Topical anesthetic Lidocaine jelly or other agent Water soluble lubricant Tape or device to secure tube Stethoscope Bag-valve device/ manual bag With reservoir Connected to oxygen at 15 L/min Optional equipment Magill forceps Oropharyngeal airway
- 20. The ET tube is passed through the mouth and vocal cords and into the trachea with the aid of a laryngoscope or bronchoscope.
- 21. The patient is placed in a “sniffing” position to align the airway structures. Placing a folded towel or bath blanket under the head may help achieve this position. If the procedure is performed electively, a topical anesthetic and/or premedication with sedative or paralytic agent may be used so that the patient better tolerates the procedure. Before the procedure is performed, the patient is hyperoxygenated and hyperventilated with 100% oxygen by use of a bag-valve device with a face mask. The proper sized tube is chosen. All ETTs is increase the work of breathing; however a tube that is too small substantially increases the work of breathing and may make ventilation and weaning difficult.
- 22. The average sized ETT used for females ranges from 7.5 to 8.0 mm, whereas the average sized ETT used for males ranges from 8.5 to 9.0 mm. After the tube is selected, the cuff on the balloon is inflated to check for proper functioning and/or any leaks. A stylet is used to stiffen the ETT and facilitate insertion. The ETT is lubricated with a water-soluble lubricant. The laryngoscope is attached to the appropriate size and type of blade (straight or curved). The choice of blades varies. The straight blade elevates the epiglottis anteriorly to expose the vocal cords. The tip of the curved blade fits into the vallecula. When upward traction is placed on the laryngoscope, the epiglottis is displaced anteriorly. The person doing the intubation inserts the laryngoscope into the mouth to visualize the vocal cords.
- 23. Excess secretions and/or vomitus is suctioned to facilitate visualization of the vocal cords; the tonsil suction tip is very efficient in removing the secretion The ETT is inserted 5 to 6 cm beyond the vocal cords, and the cuff is inflated. The procedure should be performed within 30 seconds. If the intubation is difficult, the patient should be manually ventilated between intubation attempts. Frequently, the patient requires endotracheal suctioning for removal of excess secretions immediately after intubation.
- 24. If the patient needs assistance with breathing, ventilation is achieved with either the bag-valve device or ventilator. Placement of the ETT is verified by the movement of air in and out of the tube, observation of bilateral chest expansion with inspiration and auscultation of bilateral breath sounds while the patient is ventilated with a bag-valve device. Another method for verifying tube placement is end-tidal carbon-dioxide monitoring. If th tube is in the trachea (versus esophagus), carbon dioxide is detected in exhaled air. After intubation a portable chest x-ray study is always performed for verification of the tube placement. The tip of the ETT should be approximately 2 to 5 cm above the carina. Once proper tube placement is verified, the ETT is secured with tape or another device in order to prevent dislodging.
- 25. ADVANTAGES easily and quickly performed larger tube facilitates suction and procedures such as bronchoscopy less kinking of tube DISADVANTAGES not recommended in patients with suspended cervical injury uncomfortable mouth care more difficult to perform impairs ability to gag and swallow may increase salivation may cause irritation and ulceration of the mouth
- 26. NASAL ENDOTRACHEAL INTUBATION The ET is placed blindingly (ie. Without visualizing the larynx) through the nose, nasopharynx and vocal cords. PROCEDURE FOR ORAL INTUBATION A nasotracheal ETT is usually better tolerated in an alert patient and may e easier to stabilize. In nasotracheal intubation, the ETT is usually inserted through the nares and then passed “blindly” into the glottis during inspiration. The blind intubation method is performed in the alert patient who is capable of spontaneous respirations. The nose and pharynx are anesthetized before the procedure. Nasotracheal intubation can also be performed through direct visualization. In this method, practitioners may use a laryngoscope and Magill forceps or fiberoptic bronchoscopy during the intubation.
- 27. ADVANTAGES greater patient comfort and better tolerance better mouth care possible fewer oral complication less risk of accidental extubation facilitates swallowing of secretions can administer small amounts of oral liquids if patient able to swallow DISADVANTAGES more difficult to perform may cause nasal hemorrhage and sinusitis secretion removal more difficult because of smaller tube diameter and longer tube length
- 28. Several complications may occur as a result of oral endotracheal or nasotracheal intubation. Complications include- trauma to airway structures hypoxia dysrhythmias aspiration accidental intubation of esophagus
- 29. laryngospasm bronchospasm intubation of the right mainstem bronchus an endotracheal tube that is mistakenly sized or misplaced, especially in the apneic patient, can quickly lead to hypoxia and death Broken teeth or dentures
- 30. Adequate ventilation is dependent on the free movement of air through the upper and lower airways. In many conditions, the airway becomes narrowed or blocked as a result of disease process, broncho-constriction, foreign body or secretions. Maintaining a patent (open) airway is achieved through meticulous airway management, whether in an emergency situation such as airway obstruction, or in long term management, as in caring for a patient with an endotracheal or a tracheostomy tube.