Surgency Hacking for Defense 2017
•Descargar como PPTX, PDF•
1 recomendación•129,366 vistas

mission model, mission model canvas, customer development, Hacking for Defense, lean startup, stanford, startup, steve blank, Pete Newell, Joe Felter, minimum viable product

Recomendados
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Surgency Hacking for Defense 2017
Similar a Surgency Hacking for Defense 2017 (20)
Más de Stanford University
Más de Stanford University (20)
Último
Último (20)
Surgency Hacking for Defense 2017
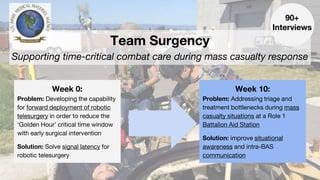
- 1. Team Surgency Supporting time-critical combat care during mass casualty response Week 0: Problem: Developing the capability for forward deployment of robotic telesurgery in order to reduce the ‘Golden Hour’ critical time window with early surgical intervention Solution: Solve signal latency for robotic telesurgery Week 10: Problem: Addressing triage and treatment bottlenecks during mass casualty situations at a Role 1 Battalion Aid Station Solution: improve situational awareness and intra-BAS communication 90+ Interviews
- 2. Chris Sebastian Software Engineering & Product Andrew DeClerck Machine Learning & Software Engineering Negin Behzadian Analog Circuit Design & Signals Abbey Cutchin Tissue Engineering & Orthopedic Surgery Mentors and Sponsors Rafi Holtzman Dr. Steve Hong Amanda Love, USAMMA The Team
- 4. 0 1 2 3 4 5 6 7 8 9 EmotionalState 10 Robotic Telesurgery ? What is the Problem? It’s a Management Problem! Who is this for? Beneficiary Buy-In Development Next Steps Our Journey
- 5. Develop capability for robotic telesurgery that would allow physicians to provide time-critical treatments for injured patients from remote geographic distances. The Original Challenge
- 6. “People are scared to move a daVinci down a hallway, let alone use it on the battlefield” - Anonymous Stanford Hospital Trauma Surgeon
- 7. 0 1 2 3 4 5 6 7 8 9 EmotionalState 10 Robotic Telesurgery ? What is the Problem? It’s a Management Problem! Who is this for? Beneficiary Buy-In Development Next Steps Our Journey
- 8. Where can we add value? Evacuation Forward CarePOINT OF INJURY Role 2 Role 3
- 9. Visit to 129th Rescue Wing at Moffett Airfield
- 10. 90% before arrival to medical treatment facility
- 11. 25% of those fatalities were deemed survivable
- 12. Where can we add value? Evacuation Forward CarePOINT OF INJURY Role 2 Role 3
- 13. “[Mass casualty triage] is not a patient care problem, it’s a management problem.” - 129th Rescue Wing Pararescuer
- 14. 0 1 2 3 4 5 6 7 8 9 EmotionalState 10 Robotic Telesurgery ? What is the Problem? It’s a Management Problem! Who is this for? Beneficiary Buy-In Development Next Steps Our Journey
- 15. Civilian Mass Casualty Training Simulation
- 16. “It’s a waste of time to try and diagnose — it’s all about prioritization.” - Timothy Browder, MD; Stanford Trauma Surgery
- 17. Justin Roberto Davis Clute Nicolas Lozano MVP 1.0 A Potential Solution for Automating Pre-Evacuation Mass Casualty Prioritization
- 18. UWB Network Zephyr Vitals Sensors Leveraging FDA-approved physiological monitoring system, already deployed in several high-stress operational environments
- 19. “The first time extensive triage takes place is at the Battalion Aid Station.” - LtCol Hasseltine, former Commanding Officer, 2d Battalion, 7th Marines,1st Marine Divison
- 20. 0 1 2 3 4 5 6 7 8 9 EmotionalState 10 Robotic Telesurgery ? What is the Problem? It’s a Management Problem! Who is this for? Beneficiary Buy-In Development Next Steps Our Journey
- 21. Battalion Aid Station? EXPECTANT STAGING AREA BLACK MEDEVAC: Medical Officer TRIAGE TREATMENT INCOMING CASUALTIES MEDEVAC To Role II/III
- 22. Current Prioritization at Battalion Aid Stations White Board TrackingTriage Card
- 23. “There is a continuous stream of communication at a BAS supporting triage, treatment, and EVAC of casualties across medical and tactical personnel. This chain could easily break down in the chaos of a mass cal.” - MAJ Michael Holloway, former BAS Physician Assistant
- 24. 0 1 2 3 4 5 6 7 8 9 EmotionalState 10 Robotic Telesurgery ? What is the Problem? It’s a Management Problem! Who is this for? Beneficiary Buy-In Development Next Steps Our Journey
- 25. MVP 2.1: Triage Manager Interface
- 26. MVP 2.2: Physician Assistant Interface
- 27. Final MVP: Evaluating Product-Mission Fit at the BAS TRIAGE TREATMENT CAS. INFO INPUT: Secondary Triage Officer OUTPUT: Physician Assistant EXPECTANT STAGING AREA BLACK SENSOR INPUT: Field Medics MEDEVAC: Medical Officer
- 28. Surgency: Mission Model Canvas - UI/UX Design MVP - Software Engineering - Interface/integrate w/ Zephyr sensors - Purchase/support Zephyr supply - Gain buy-in from JTS and incorporate in standard practice - Continued sponsorship by military beneficiary - Industry (wearable sensors, H2Care, Zephyr Technologies) - Course faculty and staff, military liaisons, DIUx, SOFWERX, In-Q-Tel - Problem Sponsors: USAMMA - DoD organization with interest in medical device research (USAMRMC, TATRC, DARPA) - Joint Trauma Registry -Primary: Physician Assistants at Role 1 BAS - Secondary: other BAS medical officers (i.e., triage medics), and potentially tactical officers - Tertiary: Care providers at higher echelons of care - Increase situational awareness: Constant vital monitoring provides PA with greater awareness of patient status. - Improve efficiency of communication among BAS roles: Augmenting PA access to communication flow from medical officer -> PA -> Platoon Sgt for quicker, more informed decisions - Improve efficiency of MEDEVACs from BAS: More accurate prioritization during MEDEVAC requests prevents unnecessary allocation of MEDEVACs and crew -Medical force multiplier: With more efficient allocation of MEDEVACs, allow for increased access to shared resources between different teams. - Improved medic-supported triage of combat injuries at POI in mass casualty situations - Widespread adoption & trust from DoD medical team and DoD command - Lives saved / Improved Quality of Care / Time to MEDEVAC / MEDEVACS sent vs patients transported - Test case in mass casualty situation with advanced medical first responders (18D trained) - Test case in mass casualty situation with standard combat medics Fixed: - Software design & engineering - Robotics/Surgery Suite Costs Variable: - Customer acquisition/sales - USAMMA procurement /sustainment resources - Medical Advisors - Testing facilities - AI/ML advisors - Need demand signal from BAS medical officers responsible for triage, treatment, and EVAC decisions - Need execution and active use by medics and first responders at BAS -Need implementation direction from DoD leadership Beneficiaries Mission AchievementMission Budget/Costs Buy-In/Support Deployment Value PropositionKey Activities Key Resources Key Partners
- 29. Value Propositions and Beneficiaries Automated Continuous Monitoring Improved Intra-BAS Communication Increased Situational Awareness @BAS Medical personnel at a BAS Care providers at higher echelons of care Increased Situational Awareness/Preparation at higher Roles of Care Tactical personnel at a BAS
- 30. “I have dozens of anecdotes of patients that have died or had poor outcomes, because the number of casualties overwhelmed capability to monitor or treat...” - LtCol DeLellis, Deputy Surgeon at the United States Army Special Operations Command
- 31. “...active monitoring would likely have changed the outcome, for the better, for many of those patients.” - LtCol DeLellis, Deputy Surgeon at the United States Army Special Operations Command
- 32. Mission Achievement: Save lives deemed survivable, where they are often lost
- 33. 0 1 2 3 4 5 6 7 8 9 EmotionalState 10 Robotic Telesurgery ? What is the Problem? It’s a Management Problem! Who is this for? Beneficiary Buy-In Development Next Steps Our Journey
- 34. Development - Data Entry Application
- 35. Development - PA Interface
- 36. Development - PA Interface
- 37. Testing our Final MVP: 23rd Marine Regiment
- 38. “[The MVP] would effectively eliminate the standard 15 minute interval between vital re-measurements by enabling continuous vitals monitoring.” - 23rd Marine Regiment Corpsman
- 39. 0 1 2 3 4 5 6 7 8 9 EmotionalState 10 Robotic Telesurgery ? What is the Problem? It’s a Management Problem! Who is this for? Beneficiary Buy-In Development Next Steps Our Journey
- 40. Internal Readiness Level Prototype of low- fidelity Minimum Viable Product
- 41. Immediate Next Steps Hacking for Defense Spring 2017 Open Source GitHub
- 42. Where do we go from here? - Secure funding sources for further development i.e. the AAMTI Award - Interface with Zephyr biopatch sensors - Work with USAMMA to develop formal requirement upon MVP screening - Explore field testing with a unit in a frequent deployment cycle i.e. the 101st Airborne
- 43. Acknowledgements: - USAMMA: Amanda Love, Jay Wang, Nita Grimsley - TATRC: Daniel Kral, James Beach, Nathan Fisher - Mentors: Steven Hong, David Zinn, George Hasseltine, Seth Krummrich, Rafi Holtzman, Tammer Barkouki - MVP Feedback: Stephen DeLellis, Jeffrey Oliver, Michael Holloway, Erwin Villeros