2. Endothelium is a largest endocrine organ.
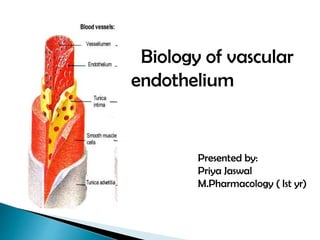
The endothelium is a thin layer of cells which lines
the interior surface of blood vessels and lymphatic
vessels forming an interface between circulating
blood and lymph in the lumen and the rest of the
vessel wall.
The cells which form the endothelium are called
endothelial cells.
Endothelial cells in direct contact with blood are
called vascular endothelial cells where as those in
direct contact with lymph are known as lymphatic
endothelial cells.
3. The basic constituents of the walls of blood vessels are
Endothelial cells
Smooth muscle cells
Extracellular matrix
Elastin
Collagen,
Glycosoaminoglycans.
The three concentric layers—
Intima,
Media
Adventitia
4. These can be vasodilatory factors such as
nitric oxide (NO),
prostacyclin (PGI2)
endothelium derived hyperpolarizing factor (EDHF)
These can be vasoconstrictive factors such as
thromboxane (TXA2)
endothelin-1 (ET-1).
5. VASODILATORS ROLE
NITRIC OXIDE • maintenance of basal vasodilator tone of the
blood vessels
• Reduce platelet and monocyte stickiness
• Reduce oxidation of LDL
• Reduce release of superoxide free radicals.
PROSTACYCLIN • It is synthesized from arachadonic acid
• It mainly involve PGI2 and PGE2
• It relaxes the vascular smooth muscle
• It helps in the release of NO from
endothelium
ENDOTHELIUM
DERIVED
HYPERPOLARIZATION
FACTOR
• Relax smooth muscle
6.
7. In 1980,Furchgott and Zawadzki first described
endothelium dependent relaxation of blood vessels by
acetylcholine.
Further studies in 1984 revealed that other factors such as
bradykinin, histamine and 5-hydroxytryptamine releases
endothelium derived relaxing factor (EDRF), which can
modulate vessel tone.
In 1988 Palmer et al could detect NO production both
biologically and chemically by chemiluminescence. The
following year in 1989 the enzyme responsible for NO
production, NO synthase, was discovered and NO
pathway was proposed.
8. A chemical compound with formula NO is a free radical
gas.
It is first identified as endothelial derived releasing
factor(E D R F ).
Nitric oxide differs from other neurotransmitter and
hormones in a way that it is not regulated by storage,
release , or targeted degradation.
NO does not require receptor for its action when
synthesized, it immediately utilized.
Ca++ calmodulin complex is necessary for nitric oxide
synthesis.
9.
10.
11. NOS I or n NOS
Central and peripheral neuronal cells, brain, spinal cord, platelets.
Ca++ dependent, used for neuronal communication
Constitutive
NOS II or I NOS
Most nucleated cells, particularly macrophages
Independent of intracellular Ca++ and its regulation depend upon de
novo synthesis.
Inducible in presence of inflammatory cytokines, bacterial
liposaccharides.
NOS III or e NOS
Present on Vascular endothelial cells and neuronal cells
Ca+2 dependent
Vascular regulation
12. Nitric Oxide plays important role in body systems :
• Relaxation of vascular smooth muscle cells.
• Inhibits platelet aggregation and adhesion.
• Plays a role in long term memory.
• Vasodilation
• Reduces leukocyte adhesion.
• NO is a powerful stimulator of cell division,maturation
and differentiation : plays role in wound healing and
tissue repair.
13. Prostacyclin (or PGI2) is a prostaglandin member of the
family of lipid molecules known as eicosanoids. It inhibits
platelet activation and is also an effective vasodilator.
In 1960s, ,Professor John Vane, began to explore the role
of prostaglandins in anaphylaxis and respiratory diseases. Sir
John discovered that aspirin and other oral anti-inflammatory
drugs work by inhibiting the synthesis of prostaglandins.
Sir John and a team had identified a lipid mediator they called
“PG-X,” which inhibits platelet aggregation.
14. .
The endothelium controls vascular tone not only by releasing
NO and prostacyclin, but also by other pathways causing
hyperpolarization of the underlying smooth muscle cells. This
characteristic was at the origin of the term ‘endothelium-
derived hyperpolarizing factor’ (EDHF).
However, this factor includes different mechanisms.
Arachidonic acid metabolites derived from the COX,
L0X and cytochrome P450 pathways, H2O2, CO, H2S and
various peptides can be released by endothelial cells.
These factors activate different families of K+ channels and
causes hyperpolarization of the vascular smooth muscle cells
contribute to the mechanisms leading to their relaxation.
15. Although the phenomenon of EDHF has been observed
and reported in scientific literature, to date the chemical
identity of the factor(s) has not been determined.
1) In some cases, members of a class of arachidonic acid
derivatives, the epoxyeicosatrienoic acids (EETs), have been
found to mediate the vasodilatation. These compounds are
formed by epoxidation of any one of four double bonds of
the arachidonic acid carbon backbone by cytochrome p450
epoxygenase enzymes.
16. 2) In some cases hydrogen peroxide has been suggested
to function as an EDHF in some vascular beds;
although this is not true in all cases,sometimes it also
causes inhibiton of K+.
3) It has been suggested that EDHF is Potassium Ions
(K+) as the activation of endothelial K+_Ca+ channels
causes an efflux of K+ from endothelial cells
towards the extracellular space.
4) Direct intercellular communication via gap junctions
allows passive spread of agonist-induced endothelial
hyperpolarization through the vessel wall. In some
arteries, eicosanoids and K+ ions may themselves
initiate a endothelial hyperpolarization.
17.
18. The endothelium not only mediates relaxation but is a
source of contracting factors.
Endothelium-dependent contractions are elicited by
physical and chemical stimuli (i.e.hypoxia, pressure,
and stretch) and autacoids, local and circulating
hormones.
Endothelin-1 (ET-1)
Thromboxane A2 (TXA2), prostaglandin H2 (PGH2)
Angiotensin- II
Reactive oxygen species(ROS); these are known to
be potent EDCF’s.
19. Prostaglandin H2 (PGH2) and Thromboxane A2
(TXA2) act primarily as vasoconstrictors.
These substances, once produced diffuse to the
underlying vascular smooth muscle cells and through
the activation of specific receptors (TP receptors)
induce contraction.
20. Endothelin-1 (ET-1) was first identified in 1988 as an
endothelial cell-derived peptide with the greatest vasoconstrictor
property.
Factors known to promote endothelin-1 production include
inflammatory mediators, hypoxia, and vascular shear stress.
Endothelin production is inhibited by nitric oxide, nitric oxide
donor drugs, and dilator prostanoids
ET-1 is a peptide secreted mostly by vascular endothelial cells,
the predominant isoform expressed in vasculature and the most
potent vasoconstrictor currently known.
21. Endothelin has three isoforms:
ET-1 ,ET-2 and ET-3.
Endothelin-1 receptors :
These are of 4 types –ETA, ETB1, ETB3, ETc
ETA mediates vasoconstriction ; found in the smooth
muscle and binding of endothelin to ETA increases
vasoconstriction.
ETB1 mediates vasodilation : When endothelin binds
to ETB1 receptors, this leads to the release of nitric
oxide.
ETB3 mediates vasoconstriction.
ETC has yet no clearly defined function
23. Antagonist-
BQ-123
FK 139317
TTA 386
Ambrisentan
Sitaxentan
Atrasentan
Zibotentan
Non peptide selective
antagonist-
PD 151242 , L 754142 ,PD
156707,
BMS 182874
SB 234551
Agonist-
sarafotoxin (aal-ET1)
BQ 3020
IRL 1620
Antagonist-
BQ 788, RO468443
IRL2500, A192621
RES 7011
Antagonist- block both
ETa & ETb
TAK 044
Bosentan
SB 209670
ETa receptor ETb receptor
24. Ambrisentan ,dose - 2.5-10mg/od used for pulmonary
hypertension.
Sitaxentan sodium (TBC-11251) is a medication for the
treatment of pulmonary arterial hypertension (PAH). In 2010,
Pfizer voluntarily removed sitaxentan from the market due to
concerns about liver toxicity.
Atrasentan is an experimental drug that is being studied for
the treatment of various types of cancer.Atrasentan blocks
endothelin induced cell proliferation.
Zibotentan (ZD4054) is an anti-cancer drug & endothelin
receptor antagonist.
It failed a phase III clinical trial for prostate cancer but other
trials are planned.
25. Angiotensin II, beyond being produced systemically,
can be released by endothelial cell and induce local
vascular constriction.
Angiotensin II constricts arteries and veins by
binding to AT1 receptors located on the smooth
muscle, which are coupled to a Gq-protein and the
IP3 signal transduction pathway.
Angiotensin II causes arterial vasoconstriction
leading to increase in B.P.
26. ROS can inhibit endothelium-dependent vasodilator
pathways [i.e. the NO pathway and the EDHF pathways]
and shift the balance in eicosanoids action from
vasodilation and antithrombosis toward vasoconstriction
and thrombosis.
Superoxide anions reduce the bioavailibility of NO,
inhibit its main target, soluble guanylyl cyclase, and
inactivate calcium-activated potassium channels.
Peroxynitrites inhibit guanylyl cyclase, superoxide
dismutases and decrease the EDHF component.
27.
28. Endothelial dysfunction is a systemic pathological state of
the endothelium (the inner lining of blood vessels) and can be
defined as an imbalance between vasodilating and
vasoconstricting substances produced by the endothelium.
Endothelial dysfunction can result from and/or contribute to
several disease processes, as occurs in
hypertension
atherosclerosis
diabetes
septic shock
Endothelial dysfunction is a major pathophysiological
mechanism that leads towards coronary artery disease and
other atherosclerotic diseases.
30. Endothelial dysfunction
Impaired
vasomotor tone Prothrombotic
state
Pro-
inflammatory
state
Proliferation in
arterial wall
Atherosclerotic lesion formation and progression
Decreased blood flow due to thrombosis and
vasospasm
CV disease events such as cardiac death,
myocardial infarction, unstable angina,
ischaemic stroke,
31.
32.
33. Control of all the known CV risk factors
Lifestyle modification. Exercise is an important lifestyle
factor that reduces cardiovascular risk , and exercise has been
repeatedly shown to improve endothelial vasomotor
function in healthy subjects and in disease states
including hypertension , congestive heart failure ,and CAD .
Dietary modification
Diets low in fat and high in fruits and vegetables have been
recommended by the American Heart Association to decrease
cardiovascular risk .
34. Oxidative stress is a central cause of endothelial dysfunction in
atherosclerosis and there has been great interest in the effects of
antioxidant therapy.
Regarding lipid-soluble antioxidants, probucol combined with lovastatin
improved coronary endothelial function in patients with CAD .
Vitamin E has been shown to improve endothelial function in patients with
multiple risk factors, particularly cigarette smoking
Lipid-lowering therapy
Reduction of plasma low-density lipoprotein improves endothelial
function.
Treatment with HMG CoA reductase inhibitors (statins) has been
consistently shown to reduce cardiovascular risk and reverse endothelial
dysfunction