
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Scurvy (deficiency of vitamin C)
Similar a Scurvy (deficiency of vitamin C) (20)
Más de rohini sane
Más de rohini sane (20)
Último
Último (20)
Scurvy (deficiency of vitamin C)
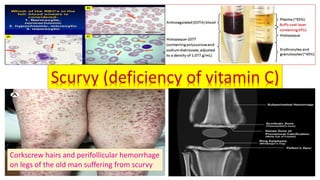
- 1. Scurvy (deficiency of vitamin C) Corkscrew hairs and perifollicular hemorrhage on legs of the old man suffering from scurvy
- 2. Biochemical functions of vitamin C in human body 1. Reversible oxidation-reduction 9. Folic acid metabolism 17. Immunological functions (immune competence) 2. Hydroxylation of Proline and Lysine 10. Amidated peptides formation (increased hormonal regulation) 18. Prevention of quick aging and Cataract 3. Collagen formation 11. Conversion of cholesterol to bile salts 19. Preventive action of chronic diseases(Anti–diabetic) 4. Bone formation 12. Biosynthesis of Corticosteroid hormones and steroid hormones 20. Preventive action of chronic diseases(Anti-cancer/anti- proliferative) 5.Tyrosinemetabolism→ Neurotransmitters (e.g..Dopamine)andCatecholamines (e.g.Epinephrine,Nor-epinephrine) 13 Carnitine biosynthesis(increased metabolic energy by α and β-fatty acid oxidation) 21. Methylation of DNA and Histone(Decreased epigenic regulation) 6. Tryptophan metabolism (Serotonin formation → Melatonin) 14. . Anti-oxidant property (response to stressful conditions) 22. Hypoxia-inducible factor (decreased gene transcription) 7. Iron metabolism 15.Sparing action of other vitamins (vitamin A and E) 23.Histamine degradation 8. Hemoglobin metabolism 16.Phagocytosis(promotesWBCsynthesis /anti-microbial/anti-sepsis) 24. Anti-radiationand protection againstozonepollution
- 3. Scurvy(deficiency of vitamin C) Name Co-enzyme form Category(years of age) RDA (mg/day) Deficiency disease Ascorbic acid No specific form Adult male(19-70 ) 90 Scurvy Women(19-70 ) 75 Pregnancy and Lactation 150 Male Infants(1-3) 15 Male Children (4-8) 40 Female infants(1-3) 45 Female children(4-8) 65 Infants up to 6 months(AI) 40 Infants up to 7-12 months(AI) 50 Adult patients receiving TPN 200 Total body pool of Human male (physiological)= 1.5 -2 g Total body pool of Human male (Scurvy) = 300mg Main reaction using the co- enzyme : Anti-oxidant property due to its reducing action ,hydroxylation of collagen.
- 4. Protracted deficiency of vitamin C leads to the classic disease of scurvy.
- 5. Causes of Scurvy( deficiency of Vitamin C) ❖Causes of scurvy : ▪ Gross dietary deficiency(unbalanced diets). ▪ Tinned food to greater extent without fresh fruits and vegetables. ▪ Infants receiving cow’s milk not supplemented. ▪ Infants receiving breast milk from deficient mother. ▪ Cooking food in frying pans, the combination of heat and large area of food in contact with air irreversibly oxidizes the vitamin c → looses its biological activity . ▪ Iron overload. ▪ Oral contraceptive pills (WBC ,platelet and ascorbic acid reduced) ▪ Infectious diseases/fever. ▪ Alcohol dependent/smokers. ▪ Mentally ill patients /renal failure patients undergoing peritoneal dialysis or hemodialysis. ▪ Oxidative stress(renal /liver diseases ,malignancies, congestive heart failure).
- 6. Symptoms of Scurvy(deficiency of Vitamin C) ❖Symptoms of scurvy: • Fragile blood vessels • Hemorrhage (petechiae →pin point Subcutaneous hemorrhages/ bleeding, periosteal due to increased capillary fragility) • Delayed wound healing, fatigue, aching muscles(due to muscle weakness) • Sore gums(swollen ,spongy ,bleeding , painful) • Poor dentine formation, pulp separated from dentine and finally teeth are lost. • Osteoid formation defective(osteoporosis) • Impaired bone formation → weak Bone →cannot withstand stress→ repeated fractures • Impaired erythropoiesis →Anemia(microcytic ,hypochromic) • Decreased immunocompetence/ immune functions • Sluggish hormonal functions of adrenal cortex and gonads Symptoms of Scurvy are related to impairment in synthesis of collagen /or the antioxidant property of vitamin C.
- 7. Clinical manifestations of Scurvy:1 • Gums: livid and swollen • Cutaneous bleeding often begins on lower thighs as perifollicular hemorrhages and large spontaneous bruises(ecchymoses) may arise almost anywhere on the body. • Ocular hemorrhage • Drying of salivary and lachrymal glands • Parotid swelling • Femoral neuropathy • Edema on lower extremities • Psychological disturbances • Anemia(microcytic, hypochromic) • Display Radiological changes characteristics of osteoporosis(Bayonet’s rib syndrome in infants). • Sudden death due to heart failure in scorbutic patients
- 8. Clinical manifestations of scurvy:2 Oral cavity in scurvy :Sore gums (swollen, spongy, bleeding and painful).Pulp is separated from dentine and finally teeth are lost . Wound healing may be delayed. Petechiae → pin point Subcutaneous hemorrhages on legs of the old man suffering from Scurvy Weak and bleeding dentine in pediatric scurvy patient Scurvy: Bleeding gums and poor dentine in an adult
- 9. Clinical manifestations of scurvy:3 Microcytic,hypochromicanemiainscurvy Corkscrew Hair (dry and coiled hair) and small bleeding near hair follicle Microcytic → size of RBCs much smaller Hypochromic → much reduced hemoglobin content
- 10. Radiological features of Scurvy ThelackofvitaminCcausesinabilitytoformadequateintracellularsubstanceinconnectivetissue andisreflectedinswollen,tenderandbleeding/bruisedlociatjoints(alsoatotherareas).
- 11. Hemorrhagic tendency in Scurvy Scurvy (ascorbic acid deficiency) Defective formation of collagen Intracellular cement substances become brittle. Capillaries are fragile. Tendency to bleed /hemorrhage under minor pressure. Manifestation of Subcutaneous hemorrhage as petechiae(mild deficiency)and as large spontaneous bruises(ecchymoses) or as hematoma(severe deficiency)
- 12. Tourniquet test for determination of hemorrhagic tendency in scurvy ➢Tourniquet test = fragility test= capillary resistance test ➢A sphygmanometer cuff is placed around the forearm and inflated. So that it compresses the venous blood flow. This pressure is kept for 5 minutes. ➢Appearance of several Petechiae hemorrhages (20 or more /6.25cm2)may seen on the forearm skin indicate Vitamin C deficiency . This is a very useful clinical test. Normal Scurvy
- 13. Tourniquet test: diagnostic test for scurvy Scurvy Normal Sphygmanometer
- 14. Internal hemorrhage in scurvy ➢In severe cases of scurvy ,hemorrhage may occur in the conjunctiva and retina. ➢Internal bleeding may be seen as epistaxis ,hematuria or melanoma. Subconjunctival bleeding Splinter Hemorrhage in nails
- 15. Infantile Scurvy (Barlow’s disease) • InfantileScurvy(Barlow’sdisease):manifestedininfantsbetween6to12monthsofage(periodinwhich weaningfrombreastmilk). • Infantilescurvydevelopswhenbabiesarebottle-fedonboiled/pasteurizedorcondensedmilk/ reconstituteddriedmilk withoutfreshfruitjuices(nosupplementationofascorbicacid). • Theprescorbuticinfantsbecomeanorexicandlistlessforfewdays. • Withthe beginningofthedisease,theinfantslieswithlegsdrawnupontheabdomen. • Theinfantscreams/crieswhentouchedespeciallywhenitslegsandarmsaremovedorlifted.Infantsexhibit bayonet’s-ribsyndrome. • Extremetenderswellingmaybefeltattheendoflongbones.Thelongbonesareacutelypainfuldueto hemorrhageunderperiosteum. • Thesternummaysinkslightlyinward. • Purpuraoccursintheskin.Thegumsareswollenandbleed. • Iftreatmentisdelayed,dyspnea,apathy,weakness,cyanosis,convulsionsanddeathmayoccur. • ThedietshouldbesupplementedwithvitaminCsources.Otherwise,deficiencyofvitaminCisseen.
- 16. Clinical manifestations of Infantile Scurvy (Barlow’s disease) Infantilescurvy(Barlow’s disease) :Extremetenderswellingmaybefeltattheendoflongbones.Thelong bonesareacutelypainfulduetohemorrhageunderperiosteum.Thesternummaysinkslightlyinward. Bayonet’s-rib syndrome Edema of lower extremities
- 17. Bachelor scurvy Bachelor or widowers scurvy : elderly bachelors and widowers who may prepare their own foods are particularly prone to development of vitamin C deficiency. In scurvy (deficiency of vitamin C ) ,patients show bruises on the limbs as a result of subcutaneous extravasation of blood due to capillary fragility.
- 18. Diagnosis of Scurvy (1) Prompt improvement following administration of vitamin C. (2) Estimation of Concentration of serum vitamin C. (2)Tourniquet test (3)Urine Ascorbic acid Saturation test : Administer 5mg of Ascorbic acid /2.5 Kg body weight orally → 50% of administered vitamin C in urine within 24 hrs.→ no scurvy (no deficiency of vitamin C) . Scurvy : 5mg Ascorbic acid /2.5 Kg body weight orally l→0 mg of vitamin C in urine within 24 hrs. (4)Intradermal test : Intradermal injection of 2,4- dichlorophenol indophenol→ determination of time required for decolorization i.e. reduction of dye. Dye detained abnormally /long persistence of blue color sub-dermally→ sub saturation of Ascorbic acid(deficiency of vitamin C).
- 19. Reference intervals of biochemical parameters related to scurvy Parameter Physiological Severe Scurvy (Microcytic, Hypochromic anemia) Total Serum Ascorbic acid ( Ascorbic acid + Dehydroascorbic acid) 0.4-1.5mg/100ml (23-85 μmol/L) < 0.2 mg /100ml(severe deficiency) (<11 μmol/L) Ascorbic acid(Leucocytes) 20-53 μg/10 6 WBC 1.14-3.01 fmols /106 WBC <10 μg/10 6 WBC < 0.57 fmols /106 WBC Urine Ascorbic acid 15-20mg/24hr 0 Buffy coat 15-25mg/100ml < 2 mg/100ml Serum iron (adult) Serum iron (children) 100 -250μg/dL (20-30μmol/L) 50-120μg/dL <100μg/dL < 45μg/dL RBC count 4.6 million / mcl < 4.1million / mcl Hemoglobin (male) Hemoglobin (female) 14-16gm/dL 13-15 gm/dL <10gm/dL Plasma/serumAscorbicacid:respondtochangesindietaryvitaminCconcentration(usedforassessment recentvitaminCintake)andpoorindicatoroftissuelevels. Laboratory independently define its own reference levels.
- 20. Hemosiderin accumulation in Scurvy ❖Hemosiderinisahemoglobin-derivedgranularpigmentandaccumulatesintissuewhenthereisalocalor systemicexcessofiron.Itisformedbypartialdeproteinizationofferritinbylysosomes. ❖Ironisnormallystoredwithincellinassociationwiththeproteinapoferritin,formingferritinmicelles. Hemosiderinpigmentrepresentsalargeaggregatesoftheseferritinmicellesbutitismoreinsolublethan ferritin.Therefore,Ironismoreslowlyreleased. ❖VisualizationHemosiderinbylightmicroscopy: 1. Goldenyelloworbrowncoloredpigment. 2. IroncanbeunambiguouslyidentifiedbyPrussianbluehistochemicalreaction. ❖ Accumulationofhemosiderin: a. Physiological:insmallamountsin mononuclearphagocytesofliver,bonemarrowandspleen. b. Pathogenic :Localexcessofiron→ hemosiderinaccumulation(e.g.hemorrhagewhenthereis extensivebreakdownofabnormal RBC(hypochromicandmicrocyticresultingfromseverescurvy). ❖ ABruise:afterlysisofRBCatthesiteofhemorrhage,theredcelldebrisisphagocytosedbymacrophages. ThehemoglobincontentiscatabolizedbylysosomeswithaccumulationofironinHemosiderin. ❖Hemosiderosispulmonis(alveolarHemosiderosis)
- 21. Deposition of hemosiderin in Scurvy Scurvy Lysis of abnormal erythrocytes (microcytic , hypochromic) The red cell debris phagocytosed by macrophages. RBC lysis →Hemoglobin from lysed RBC is catabolized by lysosomal protease→ release of iron oxide to form insoluble aggregates→ with accumulation of iron ion in Hemosiderin due to iron overload (secondary protective mechanism).
- 22. Persian blue iron stain on spleen Intra-alveolar deposition of hemosiderin Hemosiderin accumulation in Scurvy
- 23. Deposition of hemosiderin in skin in severe scurvy • Skin biopsy :deposition of hemosiderin is evident near hair follicles in patients with severe scurvy . Finegranularand clumpedironof hemosiderinstained withPrussianblue . Bruise and hemorrhage in severe Scurvy
- 24. Therapeutic use of Vitamin C ❖Vitamin C: a. can decrease the duration of cold episodes and severity of symptoms . b. enhances the synthesis of immunoglobulins and increases the phagocytic action of leucocytes. c. may act by reacting with free radicals released by phagocytic leucocytes (which become activated in infection) and decreases the inflammatory effects(cytokine storm) caused by these oxidants . Therefore vitamin C used as an adjuvant in infections (e.g.Covid19) . d. has beneficial effects in the treatment of tuberculosis. Plasma level is kept near saturation. Clinical dose is 500 mg/day. e. is recommended for treatment of ulcer ,trauma/injury and burns. ✓Except scurvy and sub-scorbutic conditions, the therapeutic use of vitamin is not specific.
- 25. Role of ascorbic acid in enhancement of immunity
- 26. Virus(COVID-19) neutralization by Ascorbic acid
- 27. The possible Beneficial effects of Ascorbic acid in management of Covid -19(?)
- 28. Toxicity of vitamin C ❖Ascorbicacidassuch,hasnotbeenfoundtobetoxicandiswelltoleratedbyhealthy subjects. ❖VitaminCbeingwatersoluble,Itisnotaccumulatedinthebody(vitaminoverload unlikely).Itisexcretedassuch,althoughasmallportionisoxidizedtoDehydroascorbicacid andthentooxalate. ❖Morethan2000mg(2000-3000mg)ofvitaminC/daypreventsinfections.But longterm useofitsmegadose,cancauseironoverload(becausevitaminChelpsinabsorptionof iron)withundesirableeffects. ❖Dehydroascorbic acid (oxidized form of ascorbic acid) is toxic.
- 29. PotentialbutrareadverseeffectsofMegadoseofvitaminC 1. cause severe gastrointestinal irritation (including nausea and diarrhea). 2. Increased oxalate excretion : Calcium salt of oxalates is major substance in kidney stones. Calcium oxalate has been implicated in the formation of kidney/urinary stones. There are controversial reports on megadose of vitamin C leading to urinary calcium oxalate stones. 3. increased uric acid excretion(aggravates gout). 4. excess iron absorption(iron overload). 5. lowers vitamin B12 levels. 6. Pro-oxidant effects in presence in the presence of free Fe 3+ or Cu 2+ . 7. Systemic conditioning. 8. Rebound ‘Scurvy” .
- 30. Megadose of Ascorbic acid and its controversy • Linus Pausing (Nobel laurate 1970) first advocated the consumption of megadose of ascorbic acid up to 18g/day (300 times the daily requirement) to prevent and cure common cold/ infections. • Keep vitamin C in gunny bags and eat in grams. • It is now clear that megadose of vitamin C dose not prevent common cold . But the duration and severity of symptoms of cold are reduced. • It is believed that ascorbic acid promotes leucocyte functions. • Megadose (1-5 g /day) of vitamin C are still continued in common cold ,wound healing ,trauma etc. and provides some health benefits. • Quick-aging process is delayed. • There are controversial reports on megadose of vitamin C leading to urinary calcium oxalate stones.
- 31. Thank You