Respiratory system Problems in GP
•
41 recomendaciones•3,621 vistas

This document provides information on respiratory problems presented by Prof. Dr. R.R. Deshpande. It discusses various respiratory issues like acute rhinitis, hoarseness of voice, acute bronchitis, chronic bronchitis, pneumonia, tuberculosis, bronchial asthma and their causes, symptoms, investigations and treatment approaches. It emphasizes the effectiveness of ayurvedic medicines for respiratory and gastrointestinal problems. It also provides differences between bronchial and lobar pneumonia, bronchial and cardiac asthma.

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (12)
Similar a Respiratory system Problems in GP
Similar a Respiratory system Problems in GP (20)
Más de rajendra deshpande
Más de rajendra deshpande (20)
Último
Último (20)
Respiratory system Problems in GP
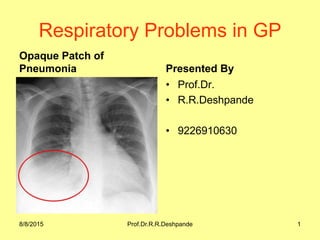
- 1. Respiratory Problems in GP Opaque Patch of Pneumonia Presented By • Prof.Dr. • R.R.Deshpande • 9226910630 8/8/2015 Prof.Dr.R.R.Deshpande 1
- 2. 8/8/2015 Prof.Dr.R.R.Deshpande 2 Respiratory Problems in GP • Presented By – • Prof.Dr.R.R.Deshpande (M.D in Ayurvdic Medicine & M.D. in Ayurvedic Physiology) • www.ayurvedicfriend.com • Mobile – 922 68 10 630 • Mailme.drrrdeshpande@rediffmail.com
- 4. 8/8/2015 Prof.Dr.R.R.Deshpande 4 Respiratory Problems in GP • 1) Acute Rhinitis • 2) Hoarseness of voice • 3) Acute bronchitis • 4) Chr bronchitis • 5) Pneumonia • 6) TB • 7) Br. Asthama • 8) Bronchieactesis • 9) Emphysema
- 5. 8/8/2015 Prof.Dr.R.R.Deshpande 5 Causes of Cough • 1) Respiratory causes • 2) Cardiac • 3) Mediastinal • 4) Drugs • 5) Miscellaneous
- 7. 8/8/2015 Prof.Dr.R.R.Deshpande 7 Investigation for Cough • 1) Haemogram ESR • 2) Stool Routine • 3) Chest X – ray (PA view) (priorly for pleurisy, pneumonia or T.B.) • 4) AFB – Acid Fast bacilli – Mycobacterium Tubercle • 5) Consecutive 3 days sputum examination is done • 6) Bronchoscopy
- 9. 8/8/2015 Prof.Dr.R.R.Deshpande 9 Medicines of Cough • 1) Allergy – Anti Allergy • 2) Antibiotic • 3) Anti tussive – dry cough • 4) Expectorant – for productive cough • 5) Mucolytic – for breaking mucoid ,sticky fibers • 6) Bronchodiator • 7) Steroids • 8) Anti-pyretic & Anti inflammatory NSAIDS • 9) Avoids Irritants • 10) Steam Inhalation.
- 10. 8/8/2015 Prof.Dr.R.R.Deshpande 10 Note Carefully • In Respiratory & GIT problems use of Ayurvedic Medicines show 80 % more better results than Allopathy • Above age – 50 years sudden change in voice and no response to treatment then refer to ENT surgeon for laryngoscopy (laryngeal cancer)
- 11. 8/8/2015 Prof.Dr.R.R.Deshpande 11 1) Allergic Rhinitis • Short attacks of severe sneezing and running of nose. • Allergen – Pollen dust • Vasomotar rhinitis – Sneezing less but blocking and running of nose. Cold remains throughout the year
- 14. Sinusitis
- 15. 8/8/2015 Prof.Dr.R.R.Deshpande 15 Treatment of Allergic Rhinitis • Tab – Zyrtec – 10 mg OD (Cetrizine) • or Tab – Lorfast – 10 mg OD (Loratidine) • These are non-sedeting drugs. • or Rhinocort Nasal Spray • or Otrivin Nasal drops (spray) • Nasivion Nasal drops / nasivion pediatric nasal drop • or Tab – Wysolone – 5 mg TDS x 5 days (Prednisolone) • Adv. – Skull Xray to rull out – DNS – Deviated Nasal Septum & Sinusitis
- 16. 8/8/2015 Prof.Dr.R.R.Deshpande 16 2) Hoarsness of Voice • Causes : • 1) Infective Laryngitis • 2) Traumatic (misuse or overuse of voice) • 3) Malignancy
- 18. 8/8/2015 Prof.Dr.R.R.Deshpande 18 2) Hoarsness of Voice -- Treatment • Advice : • 1) No talking (whispering is more dangerous) • 2) Steam inhalation (loose sticky secretion) Tr. Benzoic or vicks • Tab – Roxid – 150 mg – BD x 7 days (Roxythromycein) • Tab – Betnelan – TDS x 7 days (Betamethasone) • Tab – Gatri – 400 mg OD (Gattifloxacin) • Stops smoking
- 19. 8/8/2015 Prof.Dr.R.R.Deshpande 19 Hoarsness of Voice • Caution : • If the patient is > 50 years old No URTI, no overuse of voice, Hoarseness > 2 weeks refer to ENT, before treatment for laryngoscopy.
- 20. 8/8/2015 Prof.Dr.R.R.Deshpande 20 3) Acute Bronchitis • Clinical Features • 1) Complaining of fever : • 2) Cough with expectorant • 3) Retrosternal chest pain • O/E (on examination) Few Rhonchi and bilateral crepitations • Adv – Bed rest and stop smoking • Steam inhalation.
- 21. 8/8/2015 Prof.Dr.R.R.Deshpande 21 3) Acute Bronchitis-- Treatment • Treatment : • 1) Cap – Novamox (Amoxycillin) 500 mg QID • 2) Benadryl expectorant 1 TSF TDS (Anti allergic) • 3) Tab- Bromhexine 8 mg TDS (Mucolytic) • 4) Tab- Combiflam – 1 TDS (paracetamol) • If Dyspnoea -- Tab – Deriphylline 1 TDS (Bronchodialator)
- 23. 8/8/2015 Prof.Dr.R.R.Deshpande 23 4) Chronic Bronchitis • Complaining of – cough with expectoration – at least 2 years • O/E – Wide spread Rhonchi, basal crepitations, prolonged expiration. • Fever (only in exacerbation – attack) • Adv – X-Ray • If prominent broncho vascular makings, which indicates chr. bronchitis
- 24. 8/8/2015 Prof.Dr.R.R.Deshpande 24 Chronic Bronchitis -- Treatment • Adv – in acute exacerbation • 1) Steam inhalation • Tab – Bromhexine 8 mg TDS • If Dyspnoea / Breathlessness then • Tab – Asthalin (Salbutamol) 4 mg BDS • Tab – Bricanyl 2.5 mg TDS (Terbutalyn)
- 25. 8/8/2015 Prof.Dr.R.R.Deshpande 25 Antibiotics useful in all diseases in R.S. • 1) Cap. Mox 500 mg TDS • 2) Cap cephalexin 500 mg QID • 3) Tab- Cefuroxime – 250 mg BD (Ceftum) • 4) Tab – Levofloxacin – 500 mg OD (L – cin) • 5) Tab – Azee – 500 mg OD (Azithromycin) • 6) Tab – Bactim DS – 1 BD (very cheap antibiotic) • 7) Tab wysolone (prednisolone) 10 mg TDS if bronchospasm persists.
- 26. 8/8/2015 Prof.Dr.R.R.Deshpande 26 Chronic Bronchitis -- Treatment • After acute attack -- medicines to prevent recurrence. • 1) Tab Doxy – 1 --100 mg, 1OD (doxycycline) • 1st – 5th day of each month • 2) Cap. Novamox – 500 mg -- When the cough becomes purulent, yellow / greenish immediate start this tab 1 TDS. • Adv – 1) Stop smoking completely • 2) Avoid Irritants
- 27. 8/8/2015 Prof.Dr.R.R.Deshpande 27 5) Pneumonia • C/O – High grade fever with chills. • Cough with expectoration, unilateral chest pain, • Patient looks very toxic and ill • O/E bronchial breathing, localized crepitations, less air entry • X-Ray -- White opaque patch.
- 31. X ray of Pneumonic patch
- 32. DD of Broncho & Lobar Pneumonia Broncho pneumonia Lobar pneumonia 1) Organisms Strepto haemolyticus Diplococcus pneumonia. 2) Age Extreme of age i.e. in children and old people. Young adult 3) Pathological lesion Both lungs diffused. Limited to right lower lobe 4) Onset Insidious Acute 5) Toxemia More Less 6) Temp. Not so high but remissions High temp. & continued. 8/8/2015 Prof.Dr.R.R.Deshpande 32
- 33. DD of Broncho & Lobar Pneumonia Broncho pneumonia Lobar pneumonia 7) Signs Patchy and bilateral Unilateral, located to the right lower lobe. 8) Course (Duration) More (15 – 1 month) 7 – 10 days. 9) X-Rays Diffused finding Opaque shadow at rt. lower lobe. 10) Air entry Not specific Is less 11) Complications Common Rare 12) Treatment Antibiotics in hospital i.e. through I/V In G.P. – Antibiotics gives 8/8/2015 Prof.Dr.R.R.Deshpande 33
- 34. Pneumonia 3
- 35. 8/8/2015 Prof.Dr.R.R.Deshpande 35 Pneumonia - Treatment • Same antibiotics like the previous diseases, but Tab Roxid – covers nearly all the organism, responsible for pneumonia
- 36. 8/8/2015 Prof.Dr.R.R.Deshpande 36 Pneumonia • Caution – Pneumonia patient should be admitted in following conditions • 1) Age > 60 years • 2) Co-existing illness – DM • 3) High fever, dehydrated, toxic (Thready and feeble pulse) • I/V and antibiotics • 4) X-Ray – Shows involvement of more than 1 lobe (broncho-pneumonia) • 5) If patient refuses or unable to take medicine orally. • In addition to antibiotics also gives Tab-combiflam and Benadryl expectorant.
- 37. 8/8/2015 Prof.Dr.R.R.Deshpande 37 Breathless / Dyspnoea • 1) Respiratory causes : 80 % • 2) Cardiac causes • 3) Other • 4) Psychological
- 38. 8/8/2015 Prof.Dr.R.R.Deshpande 38 1) Respiratory causes of Dyspnoea • a) Acute Asthma • b) Acute exacerbation of COPD (chr. bronchiatis) • 3) Pneumonia • 4) Massive pleural effusion • Admit – If • 1) Pneumothorax • 2) Pulmonary embolism • 3) Pulmonary oedema / cardiac asthma / CCF
- 39. 8/8/2015 Prof.Dr.R.R.Deshpande 39 2) Cardiac causes of Dyspnoea • 2) Cardiac Causes : • a) Acute LVF • b) Valvular heart disease
- 40. 8/8/2015 Prof.Dr.R.R.Deshpande 40 3) Other causes of Dyspnoea • a) Renal failure (Uremia – breathlessness increases) Adv – Urea , Creatinine • b) Diabetic ketoacidosis / Daibetic coma
- 41. 8/8/2015 Prof.Dr.R.R.Deshpande 41 6) Pulmonary TB • Cardinal symptoms of T.B. • 1) Persistent cough with expectoration of long duration ( more than 3 weeks) • 2) Recurrent respiratory infections are common. • 3) Dyspnoea is generally not prominent at rest but is more on exertion. • 4) Cyanosis : Patients are called "blue bloaters • 5) Features of right heart failure (Cor pulmonale) are common. • 6) Chest X-ray shows enlarged heart with prominent vessels.
- 43. TB
- 44. Honeycomb Lung
- 45. 8/8/2015 Prof.Dr.R.R.Deshpande 45 Treatment of T.B. • A) Sputum positive – New Patient • HRZE for 2 months • HR x 4 months • AKT 4 1 kit per day x 2 months & cap Rcinex 100 x 4 months (Rifampicin) • clinical, radiological and pathological (sputum)
- 47. 8/8/2015 Prof.Dr.R.R.Deshpande 47 Treatment of T.B. • B) Sputum negative – New pt. • on clinical and radiological • HRZ – 2 months • HR – 4 months • Rimactazid – Z 1 kit/day x 2 months • Cap Rcinex 100 x 4 months.
- 48. 8/8/2015 Prof.Dr.R.R.Deshpande 48 Treatment of T.B. Sr. No Drug Child Dose(mg/kg /day) Adult Dose Side Effect 1 Isonex (H) 10 to 20 300 MG Neuritis,Rash 2 Rifampicin (R) 10 to 15 450 MG Hepatitis, Rash, Red Urine 3 Pyrazinamide (Z) 20 to 30 1.5 gm Hepatitis, Arthralgia
- 49. 8/8/2015 Prof.Dr.R.R.Deshpande 49 Treatment of T.B. Sr. No Drug Child Dose (mg/kg/d a) Adult Dose Side Effect 4 Ethambutol (E) 15 – 25 800 gm Optic neuritis – check vision 5 Streptomycin (S) 20 – 40 1 gm Autotoxicity (irreversible)
- 50. Progress of TB
- 51. 8/8/2015 Prof.Dr.R.R.Deshpande 51 Treatment of T.B. • Adv : • Avoid crowded places & House rest for minimum 1 month. • Restrict complete physical & mental stress. • Takes high protein diet, milk – 1 lit / day, egg, meat and Tonic like Chavanprash • Give supportive Ayurvedic treatment
- 52. DD of Bronchial & Cardiac Asthama Bronchial Asthma Cardiac Asthma 1) Pathology Bronchospasm Pulmonary congestion oedema. 2) Age Young Elderly (above 50-60 years) 3) Sex Both Male mostly 4) Past history Of Eczema, urticaria (allergy) suseptibility to cold, allergy to polon, groundnuts, eggs. No history of allergy, very few attacks, LVF, RVF 5) family history Other family members may have similar disease. Hypertension may run in families 6) personal history Highly sensitive individual Nil 8/8/2015 Prof.Dr.R.R.Deshpande 52
- 53. DD of Bronchial & Cardiac Asthama Bronchial Asthma Cardiac Asthma 7) Onset Acute, usually in early hours of morning or late hours of night. Acute usually at midnight (very specific) 8) Symptoms a) Expiratory Dyspnoea b) Expectoration – scanty & mucoid c) No palpation cough with sticky mucus. a) Both dyspnoea expi. & inspiratory b) Profuse and frothy c) Palpatation present d) lot of sputum 8/8/2015 Prof.Dr.R.R.Deshpande 53
- 54. DD of Bronchial & Cardiac Asthama Bronchial Asthma Cardiac Asthma 9) O/E in examination a) Expiratory wheez present b) sweating absent. may be present c) cyanosis absent d) pulse rate may be high e) BP normal or slightly more systolic f) Heart sounds are distant (normal) a) Absent (basal crepts and rate) b) sweating present c) Cyanosis present d) Very high (may be pulsus alterance) e) BP usually high. f) 3 heart sounds Gallop rhythm may be present in mitral area 10) Examination of lungs Plenty of wheezing bronchii. Plenty of Rales & basal crepitus 8/8/2015 Prof.Dr.R.R.Deshpande 54
- 55. DD of Bronchial & Cardiac Asthama Bronchial Asthma Cardiac Asthma 11) Treatment Antiasthematic, antiallergic, bronchodialators – Asthalin, inj – Adrenalin S/C. I/V deriphylin, inj – Amonophylin. Inj – Lasix (diuretic) I/V admit patient, inj – Aminophylin Diluted in glucose & given very slowly (for 10-15 min) Adrenalin not gives in 8/8/2015 Prof.Dr.R.R.Deshpande 55
- 57. 8/8/2015 Prof.Dr.R.R.Deshpande 57 Bronchial Asthma • 1) Asthlin inhaler (salbutamol) 2 puff • 2) Inj – Deriphyllin – 2CC • 3) or Inj. Alupent 2CC – IM/SC (orciprenalin) • 4) Inj – Salbutamol – 0.25 mg I/V slowly
- 58. Asthama inhaler
- 59. 8/8/2015 Prof.Dr.R.R.Deshpande 59 Bronchial Asthma • If patient is young • 1) Isoprenalin autohalor – 2 puff • 2) Inj – Adrenalin – 0.5 ml s/c
- 60. 8/8/2015 Prof.Dr.R.R.Deshpande 60 Bronchial Asthma • If attack is severe • Inj – Aminophyllin – 10ml -diluted in 25 % dextrose 10 ml, I/V very slowly in 5 mins • or Nebuliser – Asthalin or Ipratropium
- 61. 8/8/2015 Prof.Dr.R.R.Deshpande 61 Bronchial Asthma • C) If still not relieved with Aminophyllin • 1) Repeat inj. Aminophyllin • 2) Inj. Efcorlin – 100 mg I/V (Hydrocortisone – steroid) or inj. Decadron (Dexamethasone) • & O2 by nasal catheter.
- 62. 8/8/2015 Prof.Dr.R.R.Deshpande 62 The patient should be admitted if • 1) Patient is too breathless, to talk • 2) Pulse > 120/min • 3) RR > 30/min in children / young and in adult > 50/min. • 4) Cyanosis present – central – tongue, lips etc, peripheral – tips of fingures • 5) Bradycardia, hypotension, exhaustion • 6) Silent chest – due to complete broncho spasm (no respiratory sounds)
- 63. 8/8/2015 Prof.Dr.R.R.Deshpande 63 Maintenance of Bronchial Asthma • A) Mild intermittent Asthma : • Attack < one / week & mild • Treatment • 1) Asthalin – Inhalar – 2 puff stat. & then BD • 2) Tab – Asthalin 4 mg BD or • Tab – Deriphyllin (Theophyllin) 1 TDS • Tab – Bricanyl 5 mg BD (Terbutalin)
- 64. 8/8/2015 Prof.Dr.R.R.Deshpande 64 Maintenance of Bronchial Asthma • B) Mild Persistent Asthma : • Attack > 2 times / week, but not daily. • Treatment • 1) Asthalin – inhaler 2-3 puff. if attack occur • 2) Beclate inhaler 500 mg BD to prevent that attacks (Beclomethasone)
- 65. 8/8/2015 Prof.Dr.R.R.Deshpande 65 Maintenance of Bronchial Asthma • C) Severe Persistent Asthma • Attack daily • Treatment • 1) Beclate – inhaler – 500 mg BD • 2) Serobid inhaler – 1 puff BD • 3) Asthalin – 2-3 puffs (SOS) • Tab – Wysolone (Prednisolon) 5 mg TDS (SOS)
- 66. 8/8/2015 Prof.Dr.R.R.Deshpande 66 Kindly Note • It is proved that for the Asthmatic patient duration is not important severity of attack is important • So there is change in the concept of Status Asthamaticus
- 68. 8/8/2015 Prof.Dr.R.R.Deshpande 68 Bronchiectasis • Permanent dialation of bronchioles • Causes – Chr. respiratory diseases like chr. Brochitis • Symptoms • Cough with expectoration –Related to change of posture, hence prominent in early hours of morning or while going to bed. • Copious and purulent • Rarely haemoptysis • Chest pain recurrently, due to dry pleurisy. • febrile episode (attack) due to sec. infection.
- 69. Bronchiectasis
- 70. Vocal cords – Vicious cycle
- 71. X ray of Bronchietasis
- 72. 8/8/2015 Prof.Dr.R.R.Deshpande 72 Bronchiectasis • General symptoms: • Malaise, loss of weight • O/E -- Clubbing • Impaired Resonance – Percussion -- dull note • Vocal resonance decreases • Basal – plenty of leathery rales • X-Ray Chest (PA view) --- Thickening of basal pleura. • Bird’s nest – appearance of basal lung.
- 73. 8/8/2015 Prof.Dr.R.R.Deshpande 73 Bronchiectasis • Treatment • 1) Postural Drainage : in the morning • 2) Bronchoscopic Aspiration • 3) Antibiotics (Bed ridden pts. are kept under antibiotic cover and surgical invention is done when necessary )
- 74. 8/8/2015 Prof.Dr.R.R.Deshpande 74 Tropical Eosinophilia • C/O Intractable cough – not responding to routine treatment • Adv – PBS – for absolute Eosinophil count • IF Eosinophil is greater than 30 to 40 %
- 75. 8/8/2015 Prof.Dr.R.R.Deshpande 75 Tropical Eosinophilia • Treatment : • Tab- Hetrazan – 100 mg TDS x 1 month • Diethyl carbamazin citrate • Tab wysolone ---Tapering Dose • 1 – 1 – 1 2 days • 1 – 0 – 1 2 days • 1 – 0 – 0 2 days and then stop • Note that Antiepileptic, Antihypertensive and steroids should not be suddenly stop.
- 76. COPD
- 77. 8/8/2015 Prof.Dr.R.R.Deshpande 77 Emphysema • Definition : • Over distension of alveoli with rupture at some places – due to chr. bronchitis or chronic bronchial asthma. • Dyspnoea – exertional to begin with and then at rest also. Aggravation from time to time, due to repeated infections
- 78. 8/8/2015 Prof.Dr.R.R.Deshpande 78 Emphysema • In advanced cases dyspnoea increases, even after normal routine movements e.g. after eating, talking, defecation. • Cough with expectoration – due to associated chr. bronchitis. • Wheezing sound • Gradual weakness and loss of weight
- 79. 8/8/2015 Prof.Dr.R.R.Deshpande 79 Emphysema • Sign • 1) RR increases • 2) Central cyanosis (tongue bluish) • 3) Decubitus (special gait) -- propped up and stopping forward. • 4) Inspection : Barrel shaped chest • 5) At the line of diaphragmatic attachment, varicose veins are prominent called as • Emphysematous Girdle
- 80. 8/8/2015 Prof.Dr.R.R.Deshpande 80 Emphysema • Papation – VF (Vocal fremitus) decreases • Percussion – Hyper resonant note. • Auscultation – Breath sounds are diminished, • vesicular with prolonged expiration, VR decreases (vocal resonance)
- 81. 8/8/2015 Prof.Dr.R.R.Deshpande 81 Emphysema • X-ray – Radio translucent – lung fields, low and flat diaphragm, elongation of cardiac shadow – ‘Tubular heart’ • Complications • Right sided heart failure – chronic cor- pulmonale“( In ECG – Tall P wave – P pulmonale)
- 82. 8/8/2015 Prof.Dr.R.R.Deshpande 82 Emphysema • Treatment • 1) Breathing exercises. • 2) Antibiotics to prevent sec. infection, intermittent O2 for CCP : diuretics (Lasix) salt less diet and digitalis in CCF (gives strength to heart)
- 83. 8/8/2015 Prof.Dr.R.R.Deshpande 83 Good Experiences • Anti Allergic – • Tab Relent =cetrizine Hcl 5 mg+ Ambroxol hcl 60 mg -- 1 Tab at night
- 84. Cough ( Kasa) • Gojihvadi Kwatha 20 to 40 ml TDS • Sitopaladi Churna 5 to 10 gm TDS • Kantakaryavaleha 5 to 10 ml TDS 8/8/2015 Prof.Dr.R.R.Deshpande 84
- 85. Expectorant ( Kapha Nissarana) • Tankan Bhasma 500 mg to 1 gm TDS • Talisadi Churna --- 3 to 5 gm TDS • Vasavleha – 5 to 10 gm TDS 8/8/2015 Prof.Dr.R.R.Deshpande 85
- 86. Bronchitis ( Svasanika shoth) • Laghu malini vasant -- 2TDS • Lavangadi Churna – Half tsf tds with honey • Chousashtha Pippali churna -- Half tsf tds with honey 8/8/2015 Prof.Dr.R.R.Deshpande 86
- 87. TB ( Rajayakshma) • Raj mrigank ras – 250 mg TDS • Suvarna malini vasant – 1 tab tds • Shataputi Abhrak bhasma – 125 mg tds • Mukta panchamruta – 250 mg tds • Shilajitvadi Lauha – 500 mg tds 8/8/2015 Prof.Dr.R.R.Deshpande 87
- 88. Common cold ( Pratisyaya) • Hinguleshvara rasa 250 mg tds • Panchakola churna half tsf tds with honey • Nag guti ( very Hot) – Not for Pitta Prakruti • Cap Nesolarin ( Phyto Pharma) – Nag guti + Sameerpannag – 1 cap BD 8/8/2015 Prof.Dr.R.R.Deshpande 88
- 89. Sinusitis ( Peenas) • Shadbindu oil 3 drops TDS • Dashamula Rasayanam – 2 tsf tds 8/8/2015 Prof.Dr.R.R.Deshpande 89
- 90. Powders to treat Respiratory problems like Asthama,Cough • 1) Sitopaladi (Piitaja Kasa) • 2) Karpuradi ( Kaphaja Kasa) • 3) Talisadi ( Vataj Kasa) • 4) Chausastha Pimpali • 5) Shrungyadi • 6) Yashtimadhu • 7) Katphaladi • 8) Bhagottar 8/8/2015 Prof.Dr.R.R.Deshpande 90
- 91. Ayurvedic Tablets for Respiratory Problems • Cough --- Anandabhirav Kasa • Cold,Cough,Br.Asthama – Lavangadi vati,Naga guti,Chaturbhuja rasa,Shwas kuthar • Tuberculosis ( Rajayakshma) – Shriphalakusum vati ,Vasanta Kalpa like Suvarna malini vasant 8/8/2015 Prof.Dr.R.R.Deshpande 91
- 92. Ayurvedic Medicines for Respiratory Problems • Tubercular Lymphadenitis – Kanchanar Guggulu • Tonic in diseases like Tuberculosis, Chronic cough, Br.Asthama – Drakshasav • Cough,Br.Asthama – Kanakasav,Vasakasav,Vasadi kadha • Allergy ,Chronic sinusitis – Bhallatakadi Kadha,Bhallatakasav • Respiratory problems ( Rasayan for RS) – Chavanprash, Dhatri Rasayan, Amalaki Avaleha 8/8/2015 Prof.Dr.R.R.Deshpande 92
- 93. Ayurvedic Jams for Respiratory Problems • Cough or Haemoptysis – Vasa Avaleha, Vasa Ghruta • Chronic cough,Ch.Bronchitis – Katakaryavleha • Cough,Br.Asthama – Ardrakavleha 8/8/2015 Prof.Dr.R.R.Deshpande 93
- 94. Ayurvedic Medicines for Cough • Katphaladi or Karpuradi or Talisadi or Sitopaladi or Dadimadi or Yashtimadhu or Shrungyadi Churna • Lavangadi or Eladi or Sitopaladi Vati • Drakshasav, Punarnavasav • Agastya Hartaki avaleh,Ardrakav leh (Aalepak) ,Kantakaryav leh, Chavanprash,Vasav leh, • Vasa Ghruta, Lakshadi Tail, • Kasis bhasma, Lokanath ras, Shrunga bhasma 8/8/2015 Prof.Dr.R.R.Deshpande 94
- 95. Ayurvedic Medicines for Bronchial Asthama • Karpuradi or Dadimashtak, Pippalyadi or Yashtimadhu, Samsharkar chuna, Chausashta Pippali • Bruhatvat chintamani, Suvarna malini vasant • Kanakasav,Draksav,Dashamularishta • Swaskuthar 8/8/2015 Prof.Dr.R.R.Deshpande 95
- 96. Ayurvedic Medicines for Bronchial Asthama • Ardrakav leh, Chavanprash, • Dadimvleh, Dhatri rasayan, Lashun pak, Vasavleh, • Narayan tail • Abhrak bhasma, Manikya ras, Shrunga bhasma, Makardhwaja, Mallasindur, Rasaparpati,Rasa sindur, Loknath ras, Sameerpannag 8/8/2015 Prof.Dr.R.R.Deshpande 96
- 97. 8/8/2015 Prof.Dr.R.R.Deshpande 97 Ayurved for General Practioner • Very very popular Book in Medical Practioners • 100 common symptoms of General Practice with causes,Investigations & Ayurvedic Treatments
- 98. 8/8/2015 Prof.Dr.R.R.Deshpande 98 Clinical Examination • Systemic Examination of 8 systems • Ayurvedic Srotas Examination • Clinical significance of Lab Tests & Radiology,USG,2D Echo
- 99. 8/8/2015 Prof.Dr.R.R.Deshpande 99 Notes on Medicine Part 1 • Very very useful Book for all Medical Practioners • Guidelines with causes,symptoms,Ay urvedic & Modern Treatments to treat Fever,Pain in Abdomen & Arthritis
- 100. 8/8/2015 Prof.Dr.R.R.Deshpande 100 Best Book for Medical Students & Practioners
- 101. Preventive Cardiology & Ayurvedic Management • Best Book for GP • All cardiac problems like Hypertention,CCF, Angina,Myocardial Infarct are discussed with Ayurvedic Management Contact -922 68 10 630 8/8/2015 Prof.Dr.R.R.Deshpande 101
- 102. Digestive Problems & Ayurvedic Management • Best Book for GP • All Digestive problems like Acidity,Pain in abdomen, • Constipation ,colitis are discussed with Ayurvedic Management Contact -922 68 10 630 8/8/2015 Prof.Dr.R.R.Deshpande 102
- 103. Gynaecological Problems & Ayurvedic Management • Best Book for GP • All Gynaecological problems like Heavy bleeding,White discharge,Infertility,ca ncer are discussed with Ayurvedic Management Contact -922 68 10 630 8/8/2015 Prof.Dr.R.R.Deshpande 103
- 104. Arthritis,Backache & Ayurvedic Management • Best Book for GP • All Joint problems like Rheumatoid Arthritis,Osteoarthritis ,Backache are discussed with Ayurvedic Management Contact -922 68 10 630 8/8/2015 Prof.Dr.R.R.Deshpande 104
- 105. Neurological Problems & Ayurvedic Management • Best Book for GP • All Neurological problems like Headache,Epilepsy,Al zeimer’s Disease are discussed with Ayurvedic Management Contact -922 68 10 630 8/8/2015 Prof.Dr.R.R.Deshpande 105
- 106. Ayurvedic Concept of Diet & Nutrition • Best Book for GP • Dietary Advice according to Prakruti ,Dietary prescriptions for many diseases are given • Contact -922 68 10 630 8/8/2015 Prof.Dr.R.R.Deshpande 106
- 107. Health Tips for 365 Days 8/8/2015 Prof.Dr.R.R.Deshpande 107 • This Book is very useful from Common man to Doctors • It covers all imp aspects mentioned in Ayurveda • Open as per date & complete reading of one page only
- 108. Prof.Dr.Deshpande’s Popular Links on Internet • Just Start Internet on Desk top or Lap top or on your mobile . Copy Following Link & Paste as Web address –URL • http://www.youtube.com/user/deshpande1 959 • http://www.slideshare.net/rajendra9a/ • http://www.mixcloud.com/jamdadey/ 8/8/2015 Prof.Dr.R.R.Deshpande 108
- 109. Prof.Dr.Deshpande’s Popular Links on Internet • Just Start Internet on Desk top or Lap top or on your mobile . Copy Following Link & Paste as Web address –URL • http://professordeshpande.blogspot.in • http://professordrdeshpande.blogspot.in/ • http://www.mixcloud.com/rajendra- deshpande • https://soundcloud.com/professor- deshpande 8/8/2015 Prof.Dr.R.R.Deshpande 109
- 110. Prof.Dr.R.R.Deshpande • Sharing of Knowledge • FOR • Propagating Ayurved 8/8/2015 110Prof.Dr.R.R.Deshpande