

Recomendados
Más contenido relacionado
Destacado
Más de Katsushige Takagishi
Gim
- 1. Allergy 2007;62:1349-58 周期性発熱の鑑別診断 Syndrome 遺伝子 初発年齢 周期性発熱 炎症反応 皮疹 他の症状 治療 /発熱期間 発熱期/寛解期 PFAPA 不明 0-14yr あり/4-5d 高値/正常 稀, 様々 咽頭炎,アフタ潰瘍 ステロイド 頸部リンパ節腫脹 Cimetidine 桃切除 HIDS MVK/ 常・劣 0.5-3yr 時々/4-6d 高値/正常 丘疹 腹痛, 関節痛 コルヒチン 頸部リンパ節腫脹 IVIG, 免疫抑制 Cyclic 孤発性, ELA-2/ 0-5yr あり/3-5d 高値/正常 蜂窩織炎 口腔内潰瘍, 歯肉炎, G-CSF Neutropenia 常・優 歯周炎, 細菌感染 FMF MEFV/ 常・劣 1-20yr 無し/1-3d 高値/中等度 丹毒性 腹痛, 関節痛, 胸膜炎, コルヒチン 紅斑 アミロイドーシス TRAPS TNFr1A/ 常・優 0-53yr 無し/d-wk 高値/高値 移動性 筋肉痛, 眼周囲浮腫, ステロイド 紅斑 結膜炎, 腹痛, 関節炎 Etanercept 胸膜炎, アミロイドーシス FCAS CIAS1/ 常・優 Any 寒冷誘発 高値/正常 蕁麻疹 関節炎, 結膜炎 寒冷予防 /12hr 抗炎症 MWS CIAS1/ 常・優 乳児期 無し/様々 高値/正常 蕁麻疹 関節炎, 筋肉痛, 腹痛 抗炎症 アフタ潰瘍, 難聴, Anakinra アミロイドーシス MOMID/ CIAS1/ 常・優 新生児期 無し/持続 高値/高値 蕁麻疹 慢性髄膜炎, CNS障害 Anakinra CINCA 難聴, 失明, Eo増多 変形性関節症, 凝固障害 PFAPA; Periodic fever with aphthous stomatitis, pharyngitis, and cervical adenopathy, HIDS; Hyper-IgD syndrome FMF; Familial Mediterranean fever, TRAPS; Tumor necrosis factor receptor-associated periodic syndrome, FCAS; Familial cold autoinflammatory syndrome, MWS Muckel-Wells syndrome, NOMID/CINCA; neonatal-onset multisystem inflammatory disease/chronic infantile neutologic cutaneous and articular syndrome
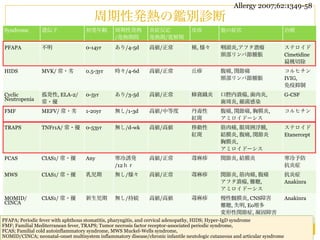
- 2. 40 Body Temperature ( Body Temperature (°C) 39 FMF vs TRAPS 39 38 FMF TRAPS 38 37 遺伝 常染色体劣性遺伝 常染色体優勢遺伝 36 37 遺伝子 0 MEFV 1 2 3 Type 1 TNF-Rに対する遺伝子 Day 発症年齢 <20歳 <20歳 36 0 1 2 3 4 5 6 7 8 9 発作期間 2日以内 14日以上 Day Jan. Feb. Mar. Apr. May June July Aug. Sept. Oct. Nov. Dec. 発熱以外の症状 漿膜炎,of丹毒様皮疹 Figure 1. Temporal Patterns Fever and Associated Clinical 結膜炎, 筋痛 Findings in a Patient with Familial Mediterranean Fever (Panel A), a Patient with the Hyper-IgD Syndrome (Panel B), and a Pa- コルヒチン反応性あり tient with the Tumor Necrosis Factor (TNF) Receptor–Associat- コルヒチンに不応 Jan. Feb. Mar. Apr. May June July Aug. Sept. Oct. Nov. Dec. 治療 ed Periodic Syndrome (Panel C). MEDICAL PROGRESS ステロイドは不応 Each panel shows the temperature during an attack of fever in ステロイド, エタネルセプトは著効 a hospitalized patient and the symptoms that accompanied the A febrile attack. The bar graph below each curve shows the num- Familial Mediterranean Fever C B TNF-Receptor–Associated Periodic Syndrome Hyper-IgD Syndrome ber of attacks that the patient had in a year, when they oc- curred, and41 their approximate duration. Serositis (peritonitis), The patient with the 41 41 Conjunctivitis, erythematous skin lesions, Cervical lymphadenopathy, vomiting, arthritis, TNF-receptor–associated periodic syndrome had long attacks myalgia and arthralgia, abdominal pain erythematous macules, Body Temperature (°C) erysipelas-like skin lesions abdominal pain, vomiting, twice in one year, whereas the patient with familial Mediterra- 40 arthralgia Body Temperature (°C) 40 the patient with the hyper-IgD syndrome had nean fever and shorter but more frequent attacks. 40 Body Temperature (°C) 39 39 38 39 38 37 tacks.17 Proteinuria (more than 0.5 g of protein per 38 24 hours)37 patients with familial Mediterranean fe- in 36 ver is highly suggestive of amyloidosis.7 0 2 4 6 8 10 12 14 16 18 20 22 24 26 36 37 Day Pathogenesis 0 and Molecular Genetic Features 1 2 3 After familial Mediterranean fever was mapped to Day the short arm of chromosome 16,18 two independent 36 groups were able to clone the gene (MEFV).19,20 The Jan. Feb. Mar. Apr. May June July Aug. Sept. Oct. Nov. Dec. 0 1 2 3 4 5 6 7 8 9 protein (pyrin, or marenostrin) encoded by MEFV Day Jan. Feb. Mar. Apr. May June July Aug. Sept. Oct. Nov. Dec. contains 781 amino acids and has a molecular weight of 86,000. MEFV is predominantly expressed in my- Figure 1. Temporal Patterns of Fever and Associated Clinical N Engl J Med 2001;345:1748-1757 eloid cells, and a Patient with Familial Mediterranean during Findings in its expression is up-regulated Fever (Panel A), a Patient with the Hyper-IgD Syndrome (Panel B), and a Pa- Jan. Feb. Mar. Apr. May June July Aug. Sept. Oct. Nov. Dec. 22
- 3. FMFの診断Criteria; Tel-Hashomer criteria Major 1項目またはMinor 2項目以上で診断 Major Minor 典型的発作* + 以下を満たす 不完全な発作** + 以下を満たす 1 非限局性の腹膜炎 1 胸膜炎, または心膜炎 2 胸膜炎(片側性) または心膜炎 2 単関節炎 3 単関節炎(股関節, 膝関節, 足関節) 3 労作後の下肢痛 4 発熱のみ 4 コルヒチンの良好な反応性 *典型発作; 38度以上の発熱が12h-3d持続. 同じタイプの発熱を3回以上繰り返す **非典型発作; 発熱が38度未満, 発作期間が6h-1wk, 腹痛発作の間に腹膜炎所見がないか, 限局性の腹膜炎. 上記の関節以外に関節炎を認める. Jpn J Clin Immunol 2011;34:355-360
- 4. FMF FMF variant * FMF 家族性地中海熱診療ガイドライン2011
- 5. Familial Mediterranean Fever Medicine 2012;91: 131-136 Allergy 2007;62:1349-58 MEFV gene @16pの異常, 小児の不定期の発熱で発症. IL-1βを誘導し, 漿膜炎を来す. 50%が4yrまでに発症, 80%が10yrまでに発症する 好発人種はnon-Ashkenazi*, ユダヤ人, トルコ人, アルメニア人, アラブ人. 特にトルコ人で最も有病率が高く, 400-1000人に1名の割合. * Ashkenazi 北欧, ドイツ在住のユダヤ人のこと. 腹痛が初発症状であることが多い. その後40度台の発熱を生じる 再発性の発熱, 漿膜炎. 症状は1-3日間持続し, 寛解期は不定. 1wk-4moで再発.
- 6. FMFで問題となるのはAA amyloidosis. 末期腎不全のリスクとなる. コルヒチンによる治療が確立される前までは, 大半の患者は<40yrでAA amyloidosisを発症し, 50yr以上まで生存する例は稀であったが, コルヒチンにより予後は改善. トルコの大学病院において1992年∼2009年に診断された FMF 650例のフォロー.(女性51%, 年齢38.6±12.6yr) その内587名(90.3%)で評価. 症状は発熱と腹膜炎が殆ど. 女性例では関節炎を呈する例が男性よりも多い(52.3% vs 43.3%, p=0.034) コルヒチンにより治療されたのは94.2%で, 平均Doseは1.5mg/d[0-3] Medicine 2012;91: 131-136
- 7. TABLE 1. Selected Demographic and Clinical 症状はほぼ全例で Characteristics of FMF Patients 発熱と腹膜炎. Patient Could Patient Not Be Contacted Contacted 胸膜炎は7割, 関節炎は4-5割, Characteristic (n = 587) (n = 63) P 丹毒様皮疹が2-3割. Female, (%) 51.4 49.2 0.791 Age at initial visit, yr 32.4 T 12.3 29.8 T 10.3 0.111 (mean T SD) Age at symptom onset, yr 14.1 T 9.1 13.2 T 8.4 0.449 (mean T SD) Age at diagnosis, yr 27.1 T 12.4 24.8 T 9.2 0.157 (mean T SD) Fever, (%) 98.6 96.6 0.228 Peritonitis, (%) 97.7 96.8 0.659 Pleuritis, (%) 68.3 69.8 0.887 Arthritis, (%) 47.8 41.3 0.353 Erysipelas-like 30.4 24.2 0.379 erythema, (%) failure due to non-amyloid kidney diseases. Three other patients had proteinuria (2 patients) or renal failure (1 patient) and de- clined biopsy. In total, 44 (7.5%) patients had renal disease. The presence of amyloidosis or renal disease was not related to age at disease onset, disease duration, types of attacks, disease severity score, colchicine usage, colchicine dosage, or M694V mutation carrier status. Data for the dates of amyloidosis and FMF diagno- Medicine 2012;91: 131-136 sis were available for 34 patients. Amyloidosis was diagnosed in 21 of these 34 (62%) patients either before or concomitantly with
- 8. FMF 587例の解析; M694V 43.9% M680I 16.2% 遺伝子検査されたのは436名. V726A 9.9% 炎症反応はESR 19.5mm/hr[2-110] CRP 0.98mg/dL[0-14.9]と軽度のことが多い. 生検にてアミロイドーシスを認めたのは37例(6.3%) 3名が無症候性タンパク尿, 12名がネフローゼ症候群, 22名が腎不全を発症. 17/22が透析. 6年間[2-10]のフォローにて, 14/587(2.4%)が死亡 死因はアミロイドーシス, 腎疾患, 加齢, 冠動脈疾患, 高血圧. アミロイドーシスは死亡HR 17.5[3.8-81.4]と死亡に関連する. Medicine 2012;91: 131-136
- 9. MFMの診断Criteria; Tel-Hashomer criteria Major 1項目またはMinor 2項目以上で診断 Major Minor 典型的発作* + 以下を満たす 不完全な発作** + 以下を満たす 1 非限局性の腹膜炎 1 胸膜炎, または心膜炎 2 胸膜炎(片側性) または心膜炎 2 単関節炎 3 単関節炎(股関節, 膝関節, 足関節) 3 労作後の下肢痛 4 発熱のみ 4 コルヒチンの良好な反応性 *典型発作; 38度以上の発熱が12h-3d持続. 同じタイプの発熱を3回以上繰り返す **非典型発作; 発熱が38度未満, 発作期間が6h-1wk, 腹痛発作の間に腹膜炎所見がないか, 限局性の腹膜炎. 上記の関節以外に関節炎を認める. Jpn J Clin Immunol 2011;34:355-360
- 10. 日本国内のFMFの報告 2009年の調査では, 患者数は292±54例 (187-398). 性別, 発症年齢の割合; 発症年齢 男性(59) 女性(75) Total(134) 0-9y 9 25 25.4% 10-19y 22 28 37.3% 20-29y 14 9 17.2% 30-39y 6 3 6.7% 40-49y 3 6 6.7% ≥50y 5 3 6.0% 発症年齢 22.5±14.4 17.2±15.7 19.6±15.3 症状頻度と海外との比較 診断時年齢 30.8±18.7 27.0±18.3 28.7±18.5 日本 トルコ イスラエル アラブ 発熱 95.5% 92% 100% 100% 腹痛 62.7% 93% 95% 94% 胸痛 35.8% 31% 43% 32% 関節痛 31.3% 47% 75% 33% 皮疹 7.5% 21% 4% 3% アミロイドーシス 3.7% 13% 27% 3% Jpn J Clin Immunol 2011;34:355-360
- 11. 日本国内の126例のMEFV遺伝子変異型 Mutation M694I/M694I 6.3% E148Q/R202Q 1.6% M694I/normal 12.7% E148Q/G304R 0.8% M694I/E148Q 19.8% E148Q/S503C 0.8% M694I/L110P 1.6% E148Q/L110P/R202Q 0.8% M694I/E148Q/L110P 11.1% E148Q/R369S/R408Q 4.0% M694I/E148Q/E148Q/L110P/L110P 0.8% E148Q/R202Q/R369S/R408Q 0.8% M680I/E148Q/L110P 0.8% E148Q/G304R/R369S/R408Q 0.8% E148Q/E148Q 0.8% R202Q/normal 0.8% E148Q/E148Q/L110P 1.6% S503C/normal 0.8% E148Q/E148Q/P369S/R408Q 1.6% E84K/normal 2.4% E148Q/normal 6.3% P369S/R408Q 4.0% E148Q/L110P 5.6% (-) 13.5% Jpn J Clin Immunol 2011;34:355-360
- 12. Exon10に変異があるものと無いものとで 漿膜炎症状, 関節炎症状の頻度が異なる. exon10 exon10 変異あり(67) 変異無し(59) 腹痛 74.6% 49.2% 胸痛 59.7% 13.6% Exon10の変異はM694I, M680I. 関節痛 22.4% 44.1% 筋痛 10.4% 13.6% アミロイドーシス 4.5% 3.4% 発症年齢 17.9±11.6y 20.6±18.3 男/女 34/33 19/40 家族歴 35.8% 13.6% Jpn J Clin Immunol 2011;34:355-360
- 13. FMF variant(不完全型FMF) 症状が非典型的なFMFで, 発熱期間が4日以上であったり, 発熱が<38度であったり, 漿膜炎発作が典型的ではなく, 関節症状, 筋症状が強かったりする. 非典型的なFMF (FMF variant)を疑った場合, 遺伝子検査が有用 MEFV遺伝子検査を行い, Exon 10の変異があればFMFと診断. Exon 10以外の変異があれば, 不全型FMFの可能性あり. exon1(E84K), exon2(E148Q, L110-E148Q, R202Q, G304R), exon3(P369S-R408Q), exon5(S503C)の変異を伴っていることがある. FMF同様にコルヒチンへの反応は良好であり, 不全型FMF, 疑い例ならばコルヒチンへの反応性を評価し, 反応あれば不全型FMFと診断する形となる. 遺伝子異常が見つからなくてもコルヒチンへの反応があれば診断. Jpn J Clin Immunol 2011;34:355-360
- 14. FMF FMF variant * FMF 家族性地中海熱診療ガイドライン2011
- 15. FMFの治療 コルヒチンが1st choice. 小児例ならば0.01-0.02mg/kg/dを分2-1で開始. 0.03mg/kg/dまで増量可 成人例ならば0.5mg/dを分2-1で開始. 1.5mg/dまで増量. コルヒチンが不応例が10%程度あり, その場合は IL-1 R拮抗薬(アナキンラ), TNF-α阻害薬(インフリキシマブ, エナネルセプト) サリドマイド が効果的との報告があり, 試される. 家族性地中海熱診療ガイドライン2011