
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Instrumental vaginaldelivery...
Similar a Instrumental vaginaldelivery... (20)
Último
Último (20)
Instrumental vaginaldelivery...
- 2. Definition: Instrumental vaginal delivery :Delivery of a baby vaginally using an instrument for assistance. The incidence of instrumental intervention varies widely both within and between countries and may be performed as infrequently as 1.5%, or as often as 26%.
- 3. FETAL Fetal distress – Altered fetal heart rate and rhythm / by passage of meconium. Objective evidence-Abnormal CTG and fetal blood sampling.
- 4. MATERNAL Inadequate expulsive efforts Prolonged second stage – More than 2 hrs without and more than 3 hrs with regional anaesthesia in a nulliparous woman. More than 2hrs with and more than 1 hr without regional anaesthesia in parous women. Maternal exhaustion Previous caesarean section or genital prolapse repair.
- 5. Medical indications to cut short second stage - Cardiac disease NYHA class III or IV Severe pre-eclampsia, eclampsia. Hypertensive crisis Uncorrected cerebral vascular malformations. Myasthenia gravis Spinal cord injury
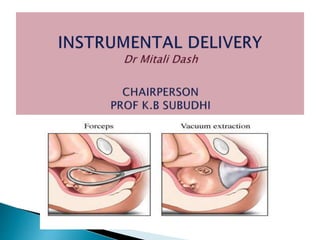
- 7. Ventouse is an instrumental device designed to assist delivery by creating a vacuum between it and the fetal scalp that creates an artificial caput or chignon within the cup that holds firmly and allows adequate traction. In the United states the device is referred as vacuum extractor , while in Europe it is commonly referred as a Ventouse.
- 9. James Yonge (1740) , a navy surgeon tried to assist delivery by using a cupping glass fitted to the fetal scalp combined with an air pump. James Simpson , (1840) a professor of midwifery in Edinburg is often credited with the invention of first vacuum extractor. Malmstrom (1954) introduced the vacuum extractor which has been widely accepted. Bird (1969) modified the cup by separating the traction device from the suction tubing allowing improved traction and preventing slippage of the cup.
- 10. TYPES OF VACUUM CUPS- Metal Semirigid-Made of flexible plastic Soft – Made of silicon. Kiwi Omnicup – Made of rigid plastic. SIZES AVAILABLE- The cups come in different sizes and are usually 4,5 or 6 cm in diameter.
- 13. KIWI OMNI CUP
- 14. The presentation should be cephalic and preferably well flexed. Membranes must be ruptured. No evidence of major cephalopelvic disproportion. .
- 15. Cervical dilatation must be sufficient to admit the cup. The larger cup is safer and more efficient. Head well engaged . In present day practice , delivery of the fetal head from high stations, i.e above +2 is no longer favoured except in the case of second twin. Obstetrician is well trained in the application of the instrument.
- 16. The patient is placed in lithotomy position. Local parts are painted with antiseptic solution such as betadine and draped with sterile sheets. Ensure that the bladder is empty.
- 17. A thorough examination to determine the station of the fetal head , position of the occiput and suture lines, assessment of the pelvis and extent of cervical dilatation made. Pudendal block anesthesia usually suffices. Proper cup placement is the most important determinant of success in vacuum extraction.
- 18. • The centre of the cup should be over sagittal suture and about 3cm in front of the posterior fontanelle • (FLEXION POINT).
- 20. Make sure that maternal soft parts like cervical rim or vaginal wall are not included in the cup. When using rigid cups vacuum is created gradually by increasing the suction by 0.2kg/cm sq every 2 mins until a negative pressure of 0.8kg/cm sq is reached . With soft cups negative pressure can be increased to 0.8kg/cm sq over as little as 1 min.
- 21. Traction should be intermittent and coordinated with maternal expulsive efforts Traction may be initiated by using a two handed technique. Fingers of one hand are placed over the suction cup while the other hand grasps the handle of the instrument.
- 22. Traction should be sustained during the pains and the direction of pull should correspond with the axis of the birth canal . This can be ensured by pulling at right angle to the cup . The higher the head the more downward should be the direction of traction.
- 23. The total duration of time recommended should not exceed 20 mins as greater the time greater is the chance of cephalhaematoma formation. It is recommended to avoid more than 3 applications to prevent complications.
- 24. After determining position of the head, (A) insert the cup into the vaginal vault, ensuring that no maternal tissues are trapped by the cup. (B) Apply the cup to the flexion point 3 cm in front of the posterior fontanel, centering the sagittal suture. (C) Pull during a contraction with a steady motion, keeping the device at right angles to the plane of the cup. In occipitoposterior deliveries, maintain the right angle if the fetal head rotates. (D) Remove the cup when the fetal jaw is reachable
- 25. Head does not descend with each pull. Head is undelivered after 3 pulls with no descent or after 20 mins of operation. The cup slips off the head with maximum negative pressure.
- 26. MATERNAL : Soft tissue injuries such as cervical tears , annular detachment of cervix , vaginal tears , perineal lacerations and tears , extension of episiotomy , vaginal wall and perineal hematomas. Traumatic PPH. Infection Incompetent os at subsequent pregnancy. Genital prolapse.
- 27. Fetal : Hypoxia , particularly when extraction has taken a long time and has been difficult. Injury to scalp , abrasions ,lacerations and cephalhaematoma. Intracranial injuries,subgaleal haemorrhage , intraventricular and cerebral haemorrhage particularly when the babies are preterm.
- 29. Neonatal jaundice. Shoulder dystocia ,particularly when the baby is macrosomic. Prolonged traction in preterm babies may lead to neurological sequel.
- 30. Premature babies , less than 34 wks of gestational maturity. Major degree of cephalopelvic disproportion. Soft tissue obstruction in the pelvis. Breech and face or non vertex presentation.
- 31. High station of the head , above station zero. Macrosomia Suspected fetal coagulopathy. Scalp electrode has been used or fetal scalp blood sampling performed.
- 33. Obstetric forceps is a pair of instruments specially designed to assist extraction of fetal head or to overcome or correct certain abnormalities in cephalopelvic relationship that interfere with progress of labor and thereby accomplishing delivery of fetus.
- 34. In modern obstetrics , all difficult forceps delivery, the high and midcavity forceps , the axis traction forceps etc. are all obsolete because of the high morbidity and mortality these instruments cause to both mother and fetus. The only permissible forceps delivery today is probably an outlet or low forceps.
- 35. INCIDENCE – 5-15% depending on the attitude of the staff, kind of labour analgesia and parity of obstetric population.
- 36. HISTORY : The credit for the design and early use of obstetric forceps goes to Chamberlen of England. This instrument was kept a family secret until Chapman publicly announced it in the late 18th century. Credit of introducing pelvic curve to the earlier design goes to Levert of Paris. Smellie gave the simple and effective design of the secure English lock.
- 37. Tarnier is remembered for his invention of the axis traction device. This permitted the pull to coincide appropriately with the axis of the pelvis at all stations. Kjelland’s forceps was designed to permit rotation and extraction of the baby. The pelvic curve was minimized and offset by a reverse pelvic at the end of the blades made it almost a straight instrument. The sliding lock permitted application of the forceps blades on an asynclitic head.
- 38. 1.Conventional traction forceps Short forceps Long forceps Long forceps with axis traction Wrigley Short Simpson Das Simpson Milne Murray’s Haige-Ferguson Neville Barnes Rotation forceps Kjelland’s Moolgaokar’s Barton’s Hay’s Forceps for special use After coming head in breech At caesarean section At caesarean section Piper’s forcep Hale
- 41. Relatively heavy. In India Das’s variety is most commonly used. Length is 37cm. Distance between tips is 2.5cm and widest diameter between blades is 9cm.
- 43. Parts are Blade, Shank, lock, handle. oBlade – Fenestrated To facilitate good grip To minimise compression of fetal head. Decreases the weight of the instrument. oToe – Tip of the blade. oHeel – End of the blade that is attached to the shank.
- 44. Pelvic curve – Fit on the axis of the birth canal (Curve of Carus). Forms a part of a circle whose radius is 17.5cm. The front of the forceps is the concave side of the pelvic curve.
- 45. oCephalic curve – Curve on the flat surface which when articulated grasps the fetal head without compression. Radius of curve is 11.5cm. oShank – part between the blade and lock. Measures 6.25cm. oLock – Requires introduction of left blade first. oHandle – Measures 12.5cm. Handles are apposed when the blades are articulated.
- 46. When articulated- Place the instrument in front of the pelvis with the tip of the blades pointing upwards and the concave side of the pelvic curve forward. The blade which corresponds to left of maternal pelvis is the left blade and that to the right side is right blade. When isolated – The tip should point upward. The cephalic curve is to be directed inwards and the pelvic curve forwards.
- 48. Most commonly used instrument for midpelvic application. Long almost straight. Absent or slight reverse pelvic curve. Has got a sliding lock which facilitates the correction of asynclitism of head. One small knob in each blade is directed towards occiput.
- 50. Lighter about 1/3rd of the weight of an ordinary long curved forceps. Instrument is short due to reduction in the length of the shanks and handle. It has a marked cephalic curve with a slight pelvic curve. Wrigley’s forceps are nearly ideal outlet forceps, light weight of length 27.5cm. The max. distance between closed blades is 7.5 and tip of blades 2.7cm.
- 51. PROCEDURE Outlet forceps CRITERIA 1 . Scalp is visible at the introitus without separating the labia. 2.Fetal skull has reached the pelvic floor. 3.Saggital suture in AP diameter or right or left occiput anterior or posterior position. 4.Fetal head is at or on perineum. 5.Rotation does not exceed 45 degrees.
- 52. Low forceps Leading point of fetal skull is at station ≥ +2 cm, and not on the pelvic floor. Rotation is 45 degrees or less (LOA or ROA to occiput anterior, and LOP or ROP to occiput posterior.) Rotation > 45 degrees.
- 53. Mid forceps High forceps Station above +2 but head is engaged. Excluded
- 54. 1 – Traction- where unaided expulsive efforts of mother are insufficient to achieve a safe delivery. 2- Rotation- KJelland’s forceps. 3 – Protection-It forms a protective cage around the preterm head. 4 – Controlled delivery of after coming head In breech to lessen the dangers of sudden decompression.
- 55. 5-Simpson forceps- Deliver the fetus with a moulded head as is common in nulliparous women. 6-Tucker-Mclane is often used for fetus with round head as often seen in multiparous women. 7-Wrigley forceps can be used in cesarean section delivery where manual traction is proving difficult.
- 56. Complex combination of traction , compression and friction by the adjacent maternal tissue. Force required for a Primipara – 18 kg. Multipara – 13 kg.
- 57. Presentation should be either occipitoanterior or direct occipitoposterior. Fully dilated cervix. Membranes already ruptured. Bladder and bowel must be empty. There must be no major disproportion at outlet.
- 58. Uterus must be actively contracting and relaxing. Head must be at perineum , rotated anteriorly such that occiput lies near or just under the symphisis pubis in occipito anterior position. The sagittal suture must lie in the anterior posterior diameter of the pelvis. Head should lie at station +2 to +4.
- 59. Cephalic application – The blades are applied along the side of the head grasping the biparietal diameter in between the widest part of the blades. The long axis of the blades corresponds to the occipito-mental plane of the fetal head. Ideal method of application as it has got a negligible compression effect on the cranium.
- 60. Biparietal-bimalar application offers uniform grip on the two sides. The sagittal suture bisects the shank which is over the flexion point – about 3 cm anterior to the occiput.
- 61. Pelvic application – When the blades of the forceps are applied on the lateral pelvic walls ignoring the position of the head, it is called pelvic application. If the head remains unrotated ,this type of application puts serious compression effect on the cranium and thus must be avoided.
- 62. 1 -Patient is taken in dorsal lithotomy position and positioned such that her buttocks are at the age of the table. 2-Proper analgesia preferably pudendal block with perineal infiltration is provided.
- 63. 3- The left blade is held vertically in the left hand over the maternal pubis. Two fingers of the right hand are slipped alongside the fetal head holding the vaginal tissues back .
- 64. 4-The blade is then introduced into the left side of the maternal pelvis under the guidance of right hand. The blade is closely applied to the fetal head , gently guided by the right fingers to sit on the lateral side of the fetal head over the baby’s ear.
- 65. • 5-The fingers of left hand are next slipped along the other side of the fetal head and the right blade is glided along its palmar aspect to the right side of the maternal pelvis.
- 66. Biparietal-bimalar application offers uniform grip on the two sides. The sagittal suture bisects the shank which is over the flexion point – about 3 cm anterior to the occiput. 6 –When correctly applied (Bimalar biparietal placement) the blades are articulated with ease.
- 67. 7-Traction is in the direction of the pelvic curve and is synchronized with contractions and maternal bearing- down efforts.
- 68. 8-An episiotomy is usually needed when the head is crowning at the vulva.
- 69. 9- In low forceps the direction of traction is initially downwards and backwards till the occiput comes under the symphysis pubis then directed horizontally straight towards operator till the head is almost crowned. The direction of pull is gradually changed upward and forward pull towards the mothers abdomen to deliver the head by extension.
- 70. In outlet forceps the direction of pull is straight horizontal and then upwards and forwards. 10-The right blade is removed first and then the left blade.
- 71. 11-IN OCCIPUTO-POSTERIOR POSITION – Traction is given horizontal till the root of nose is under the symphysis pubis then upward till the occiput emerges over the perineum and finally downwards to deliver nose and chin.
- 72. 12- IN FACE PRESENTATION – Blades are introduced along the occipito- mental diameter. Traction is applied downwards till the chin appears below symphysis pubis and then upward delivering nose , eyes , brows and occiput.
- 73. Forceps used are – Long curved with or without axis traction device & Kjelland’s forceps. INDICATION – Following manual rotation in occipito-posterior position. Blades are to be introduced only after manual correction of malposition of occiput.
- 74. Can be applied in DTA / face presentation, or correction of asynclitism. Application- Anterior blade is applied first followed by posterior blade. Wandering method in DTA – Anterior blade is applied over the face then moved over to anterior parietal bone. The posterior blade is applied between head and sacrum. Blades can also be applied directly over the parietal bones.
- 75. Named after De Lee. Refers to forceps delivery only to shorten second stage of labour when maternal and/or fetal complications are anticipated. Indications – Eclampsia Heart disease Previous H/O caesarean section Post maturity LBW To curtail the painful second stage Patient under epidural analgesia
- 76. It is a tentative attempt of forceps delivery in a case of suspected midpelvic contraction with a preamble declaration of abandoning it in favour of cesarean section if moderate traction fails to overcome the resistance. Conducted in OT keeping everything ready for caesarean section.
- 77. When a deliberate attempt in vaginal delivery with forceps has failed to expedite the process, it is called failed forceps. Causes : Incompletely dilated cervix Unrotated occipito posterior positions CPD Unrecognised malpresentation or hydrocephalus Constriction ring Clinically big baby Maternal BMI > 30 In a case with mid-cavity delivery.
- 78. Maternal complication: 1. Greater incidence of maternal vaginal and perineal lacerations including 3rd and 4th degree tears compared with vacuum deliveries. 2.Perineal pain during delivery. 3.Hematomas. 4.Postpartum hemorrhage. 5.Urinary retention. 6.Urinary and fecal incontinence.
- 79. Scalp laceration Cephalhematoma Depressed skull fracture and orbital hematoma Asphyxia Facial palsy Cervical spine injury (Rotational forceps)
- 80. Can be used in unrotated or malrotated head. Helps in autorotation. Not a space occupying device like forceps blade. Traction force is less(10KG) compared to forceps. Low rates of maternal trauma and genital tract lacerations. Analgesia need is less.
- 81. Reduced maternal pelvic floor injuries and is advocated as the instrument of first choice. Perineal injuries are less compared to forceps. Postpartum maternal discomfort are less. Simplicity of use in delivery makes it convenient to the operator.
- 82. Where moderate traction is required, forceps will be more effective as compared to ventouse. It can quickly expedite fetal delivery in case of fetal distress where ventouse will be unsuitable as it takes longer time. Safer in premature babies. The fetal head remains inside the protective cage.
- 83. Can be employed in anterior face or in after coming head of breech presentation , where ventouse is contraindicated. Lesser neonatal scalp trauma , retinal haemorrhage , jaundice or cephalohaematoma compared to ventouse. Higher rate of successful vaginal deliveries.