
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Multiple sclerosis and mysthenia gravis
Similar a Multiple sclerosis and mysthenia gravis (20)
Último
Último (20)
Multiple sclerosis and mysthenia gravis
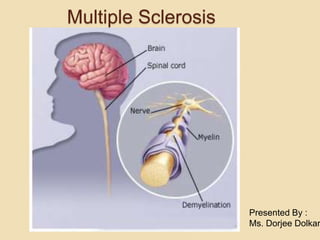
- 1. Presented By : Ms. Dorjee Dolkar Multiple Sclerosis
- 2. Multiple Sclerosis Chronic, progressive, degenerative disorder of the CNS characterized by disseminated demyelination of nerve fibers of the brain and spinal cord
- 3. INCIDENCE Usually affects young to middle- aged adults, with onset between 15 and 50 years of age Women affected more than men
- 4. Etiology Unknown cause Related to infectious, immunologic, and genetic factors
- 5. Etiology Possible precipitating factors include Infection Environmental factor-Vitamin D Immunologic reaction Sex hormone Genetic factor Poor state of health
- 7. AN AUTOIMMUNE PROCESS TRIGGERED BY GENETIC AND ENVIRONMENTAL FACTORS. INFLAMMATION OF VENULES IN THE CNS AND CAUSE DISRUPTION OF BLOOD-BRAIN BARRIER ALLOWING LYMPHOCYTES TO ENTER CNS TISSUE. THESE LYMPHOCYTES PROLIFERATE AND PRODUCE IgG WHICH RELEASE INFLAMMATORY CHEMICALS CAUSE EDEMA ACUTE ATTACK PATHOPHYSIOLOGY
- 8. REPEATED INFLAMMATORY ATTACK MYELIN IS DEMAGED AND SEGMENT OF AXON BECOME TOTALLY DEMYELINATED AND DEGENRATED ASTROCYTE PROLIFERATES IN DEMAGE REGION OF CNS ( A PROCESS CALLED GLIOSIS). PLAGUE ( GREY AND PINKISH LESION IN THE CNS). CHRONIC LESION
- 9. WHEN NERVE IMPULSE TRAVEL DOWN AN AXON DEMAGED BY MS. SLOW AND WEAK AS THEY PASS ACROSS THE DEMYLENATED AREAS. IMPULSE BLOCKED ENTIRELY WHEN AXON DEGENRATED. EXTREMITY WEAK, PARESTHESIA, VISUAL DISTURBANCES, ETC. ABNORMAL NERVE IMPULSE TRANSMISSION
- 10. Pathophysiology
- 11. Pathogenesis of MS Fig. 57-1
- 12. Multiple Sclerosis Clinical Manifestations Vague symptoms occur intermittently over months and years MS may not be diagnosed until long after the onset of the first symptom
- 13. Multiple Sclerosis Clinical Manifestations Common signs and symptoms include Visual, motor, sensory, cerebellar, and emotional problems
- 14. Multiple Sclerosis Clinical Manifestations Motor manifestations ◦ Weakness or paralysis of limbs, trunk, and head. ◦ Diplopia (double vision) ◦ Scanning speech ◦ Spasticity of muscles
- 15. Multiple Sclerosis Clinical Manifestations Sensory manifestations ◦Numbness and tingling ◦Blurred vision ◦Vertigo and tinnitus ◦Decreased hearing ◦Chronic neuropathic pain
- 16. Multiple Sclerosis Clinical Manifestations Cerebellar manifestations ◦ Nystagmus Involuntary eye movements ◦ Ataxia ◦ Dysarthria Lack of coordination in articulating speech ◦ Dysphagia Difficulty swallowing
- 17. Multiple Sclerosis Clinical Manifestations Emotional manifestations ◦Anger ◦Depression ◦Euphoria
- 18. Multiple Sclerosis Other Clinical Manifestations Bowel and bladder functions ◦Constipation ◦Spastic bladder: small capacity for urine results in incontinenceFlaccid bladder: large capacity for urine and no sensation to urinate
- 19. Multiple Sclerosis Other Clinical Manifestations Sexual dysfunction Erectile dysfunction Decreased libido Difficulty with orgasmic response Painful intercourse Decreased lubrication
- 20. Clinical Courses Of MS Relapsing- Remitting MS Primary Progressive MS Secondary Progressive MS Progressive Relapsing MS
- 21. Multiple Sclerosis Diagnostic Studies Based primarily on history, clinical manifestations, and physical examination. Certain laboratory tests are used as adjuncts to clinical exam
- 22. Multiple Sclerosis Diagnostic Studies MRI – demonstrates presence of plaques Spinal Tap / Lumbar Puncture: tested for infection. Evoked Potential Test: Monitor brain wave respond to what you see and hear.
- 23. Multiple Sclerosis Pharmacological Management Drug Therapy ◦ Corticosteroids Treat acute exacerbations by reducing edema and inflammation at the site of demyelination Do not affect the ultimate outcome or degree of residual neurologic impairment from
- 24. Cont…. ◦ Immunosuppressive Therapy Azathioprine (Imuran) Cyclophosphamide ( cytoxan) Because MS is considered an autoimmune disease Potential benefits counterbalanced against potentially serious side effects
- 25. Cont….. Antispasmotics (muscle relaxants) Baclofen (Lioresal) Dantrolene ( Dantrium) Diazepam (Valium) To relieve muscle spasm.
- 26. Multiple Sclerosis Collaborative Care Physical therapy helps Relieve spasticity Increase coordination Train the patient to substitute unaffected muscles for impaired ones
- 27. Multiple Sclerosis Collaborative Care Nutritional therapy includes megavitamins and diets consisting of low- fat, gluten-free food, and raw vegetables High-protein diet with supplementary vitamins is often prescribed
- 28. PLASMAPHERESIS: This therapy is to remove inflammatory agents such as T- lymphocytes through exchange plasma while suppressing immune response and inflammation.
- 29. Surgical Management: ACHILLES TENOTOMY: Indicated to severe spasticity and deformity. Relieve foot drop from sever plantar flexion by transected the achilles tendon.
- 30. Multiple Sclerosis Nursing Assessment Health History Risk factors Precipitation factors Clinical manifestations
- 31. Multiple Sclerosis Nursing Diagnoses Ineffective airway clearance r/t decreased cough mechanism. Risk for injury r/t blurred vision as evidenced by unable to see clearily. Altered nutrition less than body requirement r/t dysphagia as evidenced by inability to control spasticity. Activity intolerence r/t fatigue as evidenced by unable to perform ADLs.
- 33. Myasthenia Gravis “Grave Muscle Weakness”
- 35. Myasthenia Gravis Autoimmune disease affecting the neuromuscular junction Not a brain disorder – brain functions normally Characterized by fluctuating muscle weakness and fatigability Disease may be generalized or ocular specific
- 36. INCIDENCE Occurs in all races MG affects 14 per 100,000 people in the United States Can affect any age group Women – peak incidence 20's to 30's Men – peak incidence 50's to 60's Three times more common in women than men More common in asian race than other
- 37. CAUSES No single cause has been identified Abnormal thymus tissue found in most patients with MG Thymic tumors found in 15% of patients Virus infections have been found in some cases and are a suspected cause Antibodies blocking Acetylcholine.
- 38. Genetic Factors Myasthenia Gravis is not a genetically inherited disease Some families appear to carry a gene that increases the risk for developing the disease No specific gene has been identified and there are no tests for genetic screening
- 39. Exacerbation Trigger Factors Infection Stress Fatigue Cathartics (laxatives) Heat (sauna, hot tubs, sunbathing)
- 40. Pathophysiology
- 43. Signs and Symptoms Affects any of the muscles that you control voluntarily, certain muscle groups are more commonly affected than others OCULAR AND FACIAL MUSCLE: Difficulty speaking (dysarthria) Difficulty swallowing (dysphagia), Drooping eyelids (ptosis) Double vision (diplopia) Nasal-sounding speech and weak neck muscles that give the head a tendency to fall forward or backward.
- 44. Musculoskeletal System: o Weakness and Fatigue Immobility Decreased function of limbs
- 45. Respiratory System Weakening of intercostal muscle. Decreased diaphragm movement Breathlessness and dyspnea Poor gas exchange
- 46. Nutritional Dysphagia Decreased ability to move tongue Inability to feed self Weight loss Dehydration Aspiration
- 47. Cont….. Symptoms tend to progress over time, usually reaching their worst within a few years after the onset of the disease Worsening muscle weakness with repeat activity
- 48. Diagnosis test Edrophonium test (Tensilon) Antiacetylcholine receptor antibody serum level Pulmonary Function Test Single-fiber electromyography (EMG) Imaging scans Eg: CT or MRI
- 49. Tensilon Test Injection may result in a sudden, although temporary, improvement in muscle strength — an indication of myasthenia gravis. Acts to block an enzyme that breaks down acetylcholine, the chemical that transmits signals from nerve endings to muscle receptor sites.
- 50. Diet/Nutrition Eat small meals and snacks five to six times a day Avoid using low fat or diet products when possible Avoid eating lemons or tonic water Eat warm rather than hot food Runny or puree diet when swallowing is difficult Alternate sips of liquid to avoid food from sticking AVOID eating chewy or dry crumbly foods
- 51. Medications/Treatment Immunosuppressive Therapy Prednisone Azathioprine Acetylcholinesterase Inhibitors First line of therapy Neostigmine bromide (Pyridostigmine) Edrophonium chloride (Tensilon)
- 52. Surgical Management Thymectomy Removal of thymus gland. • Recommended to those who gets dysphagia due to thymus gland. • Thymus tumor
- 53. Nursing Diagnosis: Risk for injury r/t ptosis as evidenced by loss os motor control. Ineffective airway clearance r/t nonproductive cough as manifested by decreased rib cage movement. Impaired swallowing r/t fatigue and dysphagia as manifested by unable to swallow food.
- 54. Cont.. Impaired social interaction r/t change in body image as evidenced by decreased motor function. Fatigue r/t increased energy need for muscle movement as evidenced by unable to perform ADL’s. Ineffective therapeutic regimen r/t insufficient knowledge as evidenced by depression and potential for complication.
- 55. Myasthenic Crisis VS. Cholinergic Crisis Myasthenic Crisis Under medication Increased HR/BP/RR Bowel and bladder incontinence Decreased urine output Absent cough and swallow reflex May need mechanical ventilation Temporary improvement of symptoms with administration of Tensilon Cholinergic Crisis Overmedication Decreased BP Abd cramps N/V, Diarrhea Blurred vision Pallor Facial muscle twitching Constriction of pupils Tensilon has no effect Symptoms improve with administration of anticholinergics (Atropine)
- 56. Patient Teaching Teach patient/family disease process, complications, and treatments Teach patient about their medications uses dosage etc Teach medications to use with caution d/t muscle exacerbation Beta blockers, calcium channel blockers, quinine, quinidine, procainamide, some antibiotics, neuromuscular blocking agents Avoid certain medications D-penicillinamine, A-interferon, botulinum toxin
- 57. Cont…….. Teach of both Myasthenic Crisis and Cholinergic Crisis Help patient plan daily activity to coincide with energy peaks Stress need for rest periods Explain that exacerbations, remissions, and daily fluctuations are common Avoid strenuous exercise, stress, infection, exposure to hot or cold temperatures Teach patient to wear medic-alert bracelet
- 58. Prognosis Chronic disease with periods of exacerbation and sometimes remissions Disease course is highly variable Symptoms respond well to treatment and in most cases the patient can live a normal or nearly normal life Ocular Myasthenia has the best prognosis
- 59. SUMMARY