DCIS Breast Cancer
•Descargar como PPTX, PDF•
36 recomendaciones•16,731 vistas

Understanding and Treating DCIS (ductal carcinoma in situ) of the Breast

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a DCIS Breast Cancer
Similar a DCIS Breast Cancer (20)
Más de Robert J Miller MD
Más de Robert J Miller MD (20)
Último
Último (20)
DCIS Breast Cancer
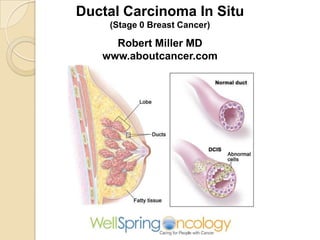
- 1. Ductal Carcinoma In Situ (Stage 0 Breast Cancer) Robert Miller MD www.aboutcancer.com
- 2. 20% of breast cancers in the US are stage 0 or noninvasive (ducal carcinoma in situ DCIS or lobular carcinoma in situ LCIS)
- 3. Age Distribution For In Situ versus Invasive NCDB Data 30 25 20 15 In Situ Invasive 10 5 0 30 40 50 60 70 80
- 4. Observed 5 Year Survival Breast Cancer 2003-2006 NCDB 100 90 80 70 60 50 40 30 20 10 0 Stage 0 Stage I Stage II Stage III Stage IV
- 5. What You Need to Know About Breast Cancer Before Deciding on Treatment • Understand the basic anatomy (lobules, ducts and lymph nodes) • Biopsy or pathology report tell you about the biology (how aggressive) of the cancer • Breast imaging studies (mammograms or ultrasound) CT, MRI, PET • Stage (particularly lymph node status)
- 9. Earliest form of cancer is often DCIS (ductal carcinoma in situ) then it progresses to invasive ductal carcinoma
- 10. ductal cells ductal carcinoma In situ (DCIS) Invasive ductal carcinoma
- 11. Normal duct cells inside a milk duct
- 12. Basement Membrane DCIS Cancer cells are confined within the milk duct basement membrane so still in situ or non-invasive Normal Duct cells Cancer Cells
- 13. Basement Membrane Invasive Cancer Once the cells have invaded through the basement membrane and outside the duct it is called invasive or infiltrating Normal Duct cells Cancer Cells
- 14. Pathology View of Ductal Carcinoma In Situ
- 15. Lymph Nodes supraclavicular Internal mammary axillary DCIS should not spread to the lymph nodes unless there is some invasion (may be focal micro-invasion) but 10 to 20 percent of lesions interpreted as DCIS on a core biopsy are upgraded to invasive cancer after excision
- 16. DCIS Ductal Carcinoma In Situ DCIS Wall of the duct
- 18. Understanding a Pathology Report 1. Invasive or Not (DCIS, LCIS) 2. Histology: what type of cancer 3. Grade: fast or slow growing 4. Hormone Receptors: is it sensitive to estrogen or progesterone 5. HER2 (human epidermal growth factor receptor 2) a genetic mutation
- 19. Imaging The cells often die in place (necrosis) and then calcify. The radiologist is looking for abnormal areas of calcification
- 20. Mammograms often show areas of calcification, which can be benign or malignant Ninety percent of women with DCIS have microcalcifications on mammography and DCIS accounts for 80 percent of all breast cancers presenting with calcifications
- 21. Mammograms In ductal carcinoma in situ (DCIS), there is normally no mass but just an area of calcification (very small areas called microcalcifications)
- 22. Microcalcifications can be very subtle Biopsy of this area showed 8mm DCIS
- 23. Biopsy = DCIS with focal micro-invasion
- 24. fat gland Larger area of microcalcifications may have invasive cancer Path = 2.9 cm area of high grade DCIS plus invasive ductal cancer
- 25. Looking for advice on treatment decisions for ductal carcinoma in situ of the breast
- 26. Treatment Decisions with DCIS 1. Surgery: total mastectomy versus conservation (lumpectomy) and ? nodes 2. Adjuvant Therapy: hormone therapy or as preventative strategy 3. Radiation: whole breast or can it be skipped
- 27. Treatment Decisions The woman should be assisted by a multidisciplinary team, including a surgeon, possibly a plastic surgeon, medical oncologist and a radiation oncologist
- 29. NCCN.org
- 34. Complete axillary lymph node resection should not be performed in the absence of evidence of invasive cancer or proven metastatic disease in women apparent pure DCIS. However, a small proportion of patients with apparent pure DCIS will be found to have invasive cancer at the time of their definitive surgical procedure. Therefore, the performance of a sentinel lymph node procedure should be strongly considered if the patient with apparent pure DCIS is to be treated with mastectomy or with excision in an anatomic location compromising the performance of a future sentinel node procedure.
- 35. Deciding on Surgery Lumpectomy Total Mastectomy The risk of cancer-related death in women with DCIS is low, estimated at 1.9 percent within 10 years. Mastectomy is curative for over 98 percent of patients with DCIS. Disease recurrence is rare after mastectomy (1 to 2 percent)
- 36. Breast Conservation Lumpectomy (remove the cancer with a small rim of normal tissue, clear margins) Sentinel node biopsy occasionally will be performed at the same time
- 37. At the time of the lumpectomy the surgeon tries to remove the cancer with a margin of normal breast tissue around the mass X-ray image of the lumpectomy specimen
- 40. Long-term outcomes of invasive ipsilateral breast tumor recurrences after lumpectomy in NSABP B-17 and B-24 randomized clinical trials for DCIS. Local Relapse in the Breast Over 15 Year Follow Up Lumpectomy Alone 19.4% Lump + Radiation 8.9 – 10% Lump + Radiation + Tamoxifen 7.3% Survival was the same in all groups Natl Cancer Inst. 2011;103(6):478.
- 41. Breast-Conserving Treatment With or Without Radiotherapy in Ductal Carcinoma In Situ: 15-Year Recurrence Rates and Outcome After a Recurrence, From the EORTC 10853 Randomized Phase III Trial JCO. 2013.49.5077
- 42. Fifteen-year results of breast-conserving surgery and definitive breast irradiation for the treatment of ductal carcinoma in situ of the breast. Cause specific survival Over all survival Years JCO Mar 1, 1996:754-63
- 43. Whole breast radiation following lumpectomy reduces the recurrence rates in DCIS by about 50%. Approximately half the recurrences are invasive and half are still DCIS. A number of factors determine the local recurrence risk: palpable mass, large size, higher grade, close or involved margins, and age < 50y. If the patient and physician view the individual risk as “low” some patients may be treated with excision alone. All data evaluating the three local treatments (lumpectomy alone, lumpectomy plus radiation or total mastectomy) show no difference in patient survival.
- 44. Van Nuys Index for Treatment of DCIS Score #1 #2 #3 Path Other Comedo Size <15mm 16-40mm High Grade >40mm Margins >10mm 1-9mm < 1mm Score 3 – 4 : Lumpectomy alone (local control is 100% vs 97%) Score 5 – 7: Lumpectomy + Radiation (local control from 68% up to 85%) Score 8-9: Mastectomy Cancer 1996 Jun 1;77(11):2267-74
- 45. Van Nuys Index for Treatment of DCIS Score #1 #2 #3 Path Other Comedo Size <15mm 16-40mm High Grade >40mm Margins >10mm 1-9mm < 1mm Score 3 – 4 : Lumpectomy alone (local control is 100% vs 97%) Score 5 – 7: Lumpectomy + Radiation (local control from 68% up to 85%) Score 8-9: Mastectomy Cancer 1996 Jun 1;77(11):2267-74
- 46. Updated Van Nuys Prognostic Index Parameter 1 Point 2 Points 3 Points Size <15mm 16-40mm >40mm Grade 1/II 1/II Necrosis III Margin 10mm 1-9mm <1mm Age >60 40-60 <40 4,5, 6 = Lumpectomy Alone 7, 8, 9 = Lumpectomy + Radiation 10, 11, 12 = Mastectomy 2003 Update PMID 14682107 -- "An argument against routine use of radiotherapy for ductal carcinoma in situ." (Silverstein MJ, Oncology (Williston Park). 2003 Nov;17(11):1511-33; discussion 1533-4, 1539, 1542 passim.)
- 47. Online Breast Cancer Calculators http://aboutcancer.com/breast_calculators.htm http://www.mskcc.org/cancer-care/adult/breast/prediction-tools
- 51. CT scan is obtained at the time of simulation CT images are then imported into the treatment planning computer. Note that at the time of the simulation the patient may receive 3 small tattoo marks
- 52. Computer generated anatomy images that will identify all the important structures to be sure the radiation covers the area of breast cancer and limits the dose to other areas
- 55. Radiation beam skims over the surface of the chest wall, ribs and lung
- 56. External Beam Radiation Monday through Friday for 5 weeks
- 57. Radiation Fields After a lumpectomy the whole breast is radiated for about 5 weeks (the red box) and then a boost dose (5 – 7 treatments) is given to the lumpectomy site (blue circle)
- 58. The whole breast treated 26 to 28 times The lumpectomy site is then treated 5 to 7 times
- 59. Short Term Side Effects of Breast Radiation Generally the side effects of breast radiation do not become noticeable until the woman has received about 10 to 15 treatments, and then become somewhat more noticeable through the rest of the treatment. The most common side effects: •skin irritation - the skin that is radiated gets red, itchy and may blister (like a sun burn) may lose hair in arm pit (biafine, prutect, myaderm, aquaphor, silvadene, triamcinalone, Radiaderm) •breast or chest wall tenderness or mild pain •tiredness or fatigue (some women feel a little lightheaded) •are swelling or edema
- 60. Long Term Side Effects of Breast Radiation • Arm swelling or lymphedema is probably less than 3% • Lung inflammation (pneumonitis) is 5% or less • Risk of rib fracture is less than 3% • Risk of nerve damage (brachial plexopathy) < 1% • Radiation fibrosis to breast • Risk of causing a new cancer is less than 1%
- 62. DCIS BREAST CANCER Robert Miller MD www.aboutcancer.com