Managing Gout: Treatment and Prevention Strategies
•Descargar como PPTX, PDF•
14 recomendaciones•3,235 vistas

Gout is a metabolic disorder caused by hyperuricemia, or high levels of uric acid in the blood. It most commonly affects middle-aged men and causes sudden, severe pain and inflammation in joints like the big toe. Acute gout occurs when uric acid crystals form in a joint, while chronic gout results in long-term joint damage. Treatment involves medications like NSAIDs, colchicine, corticosteroids, and allopurinol to reduce pain and prevent further attacks by lowering uric acid levels. Lifestyle changes like diet modification and exercise can also help prevent gout flares.

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Managing Gout: Treatment and Prevention Strategies
Similar a Managing Gout: Treatment and Prevention Strategies (20)
Más de Health Forager
Más de Health Forager (11)
Último
Último (20)
Managing Gout: Treatment and Prevention Strategies
- 1. BY, VISHWANATH GOUDA 1st M. Pharm Dept. of Pharmacy Practice NGSMIPS, Nitte University Mangaluru, 57018
- 2. INTRODUCTION Gout is the most common inflammatory joint disease. The prevalence of gout has increased over recent decades. One of the oldest recognised disease and was identified in 2460BC. Gout is normally the result of an Interaction between genetics and environmental risk factor.
- 3. DEFINATION Gout is a metabolic disorder characterized by hyperuricemia which occurs due to defective purine metabolism. Hyperuricemia can lead to deposition of sodium urate crystals in the tissues especially in joints and kidney. TYPES Acute it manifests as sudden onset of severe inflammation in a small joint due to precipitation of urate crystals in joint spaces. Chronic When pain and stiffness persist in a joint between attacks, gout become chronic
- 4. EPIDEMIOLOGY Gout is one of the oldest disease and was identified by Egyptians. Gout is a condition that most frequently affects middle aged men with only approximately 5% of the cases occurring in women. Most women with gout have a family history of disease, studies in men have failed to detect a significant genetic component. Disease of the ‘KINGS’ Rich foods have a higher concentration of protein. This could cause major problems for a person afflicted with gout
- 5. ETIOLOGY Gout occurs due to defective purine metabolism in which uric acid is the end product. The main cause of hyperuricemia occurs due to following reasons. Over production of uric acid. *Excessive turn over of nucleoproteins *Excessive dietary purines *Excessive synthesis of uric acid due to rare enzyme mutation defects. Under excretion of uric acid *Defect in renal excretion *Inborn errors of metabolism
- 7. CLINICAL PRESENTATION SYMPTOMS • Severe pain, swelling and warmth in the affected joints. • The attack is usually monarticular and the most common sites are the metatarsophalangeal and knee joints. SIGNS • Affected joints are warm, red and swollen • Mild fever may be present • Tophi may be present in chronic, severe disease
- 8. Acute Gout: Acute gout is a painful condition that typically affects only one or a few joints. The big toe, knee, or ankle joints are most often affected. Throbbing, crushing, or excruciating pain Joint appears warm and red. Fever may be there. The attack may go away in a few days, but may return from time to time. Additional attacks often last longer.
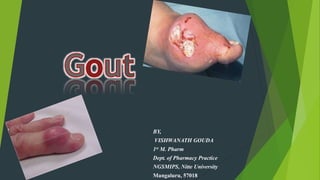
- 12. Chronic Gout Signs and symptoms include: Joint damage Loss of motion in the joints Joint pain and other) symptoms most of the time, throughout the day Skin over the deposits develops sores ((ulcers)) exuding a white pus ((chalky)) Joint stiffness ((limited motion of the affect joint)) Articular cartilage may be destroyed resulting in joint deformities Patients may develop large Subcutaneous Tophi ((Porous Stones)) in pinna of external ear, eyelids, nose, around joints, fingers, knees, at the tips of the elbows, tendons, cartilages, soft tissues as flexors in the forearms and rarely in the vocal cord and around the spine
- 13. Gouty Nephropathy The precipitation of uric acid in the renal medulla with formation of characteristic tophi was believed to evoke an inflammatory response leading to fibrosis, a loss of nephrons, and ultimately to the piece de resistance, chronic irreversible renal failure
- 14. DIAGNOSIS Physical examination and medical history Examination and analysis of synovial fluid
- 15. TREATMENT NON-PHARMACOLOGICAL THERAPY Local ice application is the most effective therapy.
- 16. PHARMACOLOGICAL THERAPY For acute gout NSAIDs Colchicine Corticosteroids For chronic gout Uricosurics • Probenecid • Sulfinpyrazoe Synthesis inhibitors Allopurinol Febuxostat
- 19. NSAIDS: • Inhibits pain & inflammation. • Inhibits urate crystal phagocytosis by decreasing the migration of granulocytes into the inflammatory area. Indomethacin : 50mg three times daily Std dose : 50mg Etodolac : 300mg twice daily Std dose : 300-500mg twice daily Ibuprofen : 400mg three times daily Std dose : 400-800mg three to four times daily.
- 20. CORTICOSTEROIDS corticosteroids are equivalent to NSAIDs in the treatment of acute gout flares They can be used either systemically or by intraarticular injection If only one or two joints are involved, either intraarticular or oral corticosteroids are recommended. If an attack is polyarticular, systemic therapy is necessary. Prednisone : 0.5mg/kg daily for 5-10days Intramuscular : Triamcinolone acetonide 60mg IM once ; methylprednisolone 100mg IM once. Intraarticular : triamcinolone acetonide 10mg large joints and 5mg small joints Corticotropin : 40units IM or SC every 72 hrs.
- 21. COLCHICINE: • Produces its anti-inflammatory effects by binding to the intracellular protein tubulin, preventing its polymerization leading to the inhibition of leukocyte migration into affected area. • Inhibits the synthesis & release of leukotrienes. Oral colchicine (Colcrys) : 1.2mg initially, followed by 0.6 mg 1 hour later
- 22. URICOSURIC AGENTS: • Probenecid • They are weak organic acids . • Sulfinpyrazone is a metabolite of phenylbutazone. • Increase the excretion of Uric acid. Probenecid : 250mg twice daily for one week. std dose : 500-250mg/day
- 23. XANTHINE OXIDASE INHIBITORS Allopurinol/ Febuxstat: • Inhibits synthesis of uric acid by inhibiting xanthine oxidase enzyme Uric acid is produced by Xanthine and Hypoxanthine by Xanthine Oxidase Inhibitor. Uric Acid is more toxic than either xanthine or hypoxanthine. Allopurinol : 100mg daily Std dose : 100-800mg/daily Febuxostat : 40mg daily Std dose : 40-80mg daily
- 28. • Interaction with warfarin • Contraindicated in: • Renal disease • PUD • GI bleeders NSAIDS • Not as effective “late” in flare • Contraindicated in dialysis patients • Cautious use in : • Renal or liver dysfunction • Active infection • Age > 70 Colchicine • Worse glycemic control • May need to use mod-high doses Corticosteroids
- 29. PREVENTION Avoiding excessive intake of purine-rich foods Maintain a healthy body weight by Exercise Restrict your intake of alcohol, especially beer ((high in Guanosine)) Avoid foods rich in fructose and sucrose which result in hyperuricemia Avoid diuretic foods or drugs which increase urination Avoid diet low in potassium ((good sources are tomatoes, potatoes, bananas, soybeans, brown rice)) since a deficiency increases blood urate Avoid consuming too much acid-containing substances Maintain an adequate intake of Vitamin C, since it has been demonstrated to increase excretion of uric acid Drink plenty of water to dilute and assist urate excretion Avoid prolonged exposure to low temperature
- 30. Reference Dipiro JT, , Talbert RL, Yee GC, Matzke GR, et al. Pharmacotherapy ; A Pathophysiologic approach. 9th edition.USA. M CGraw Hill publication2014. chapter74 Gout and Hyperuricemia, P: 1505-1520 Walker R and Whittlesea C. Clinical pharmacy and therapeutics. In Cockwell P, Strringer S and Marriott J; editor. Gout and hyperurecemia. Gret Britain; Churchhill livingstone; 5th edition; 848-857.