
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Hernia
Similar to Hernia (20)
Recently uploaded
Recently uploaded (20)
Hernia
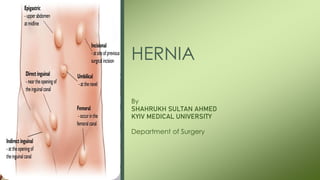
- 1. HERNIA By SHAHRUKH SULTAN AHMED KYIV MEDICAL UNIVERSITY Department of Surgery
- 2. Topics to Be Covered • Definition of Hernia • Parts of Hernia • Classifications of Hernia • Etiology, Development & Treatment of Different Types of Hernias • Acute & Chronic Complications of Hernia
- 3. Definition • Hernia means “ To Protrude “. • Hernia is defined as an abnormal protrusion of a viscus or a part of a viscus through an opening, artificial or natural with a sac, covering it.
- 5. Parts of Hernia Hernia Comprises of : Covering: Are the layers of Abdominal Wall through which sac passes. Sac: Is a diverticulum of peritoneum with mouth, neck, body & fundus. Content: Can be Omentum, Intestine, Ovary Meckel’s Diverticulum
- 7. Classification : Clinical • Reducible • Irreducible • Obstructed • Inflamed • Strangulated
- 8. Classification : Based on Sites • COMMON HERNIAS • INGUINAL ( 73% ) • INCISIONAL • FEMORAL ( 17% ) • UMBILICAL ( 8.5% ) • EPIGASTRIC
- 10. INGUINAL HERNIA • 73% of all Hernias are Inguinal Hernia • An Inguinal Hernia is a protrusion of abdominal-cavity contents through the Inguinal canal. • Male : Female : 20 : 1
- 11. Surgical Anatomy • BOUNDARIES OF INGUINAL CANAL • Anterior: External oblique aponeurosis and a few fibres of the conjoined muscle (especially of internal oblique) laterally. • Superior: Arched fibres of the conjoined muscle. • Inferior: Inguinal ligament and the lacunar ligament on the medial side (Gimbernat's ligament). • Posterior: Fascia transversalis and the conjoined tendon medially.
- 13. SURGICAL ANATOMY CONTENTS OF INGUINAL CANAL Spermatic Cord in Males Round Ligament in Females Ilioinguinal Nerve
- 14. Surgical Anatomy Hesselbach's triangle • It is bounded • Medially by lateral border of Rectus Abdominus Muscle, • Laterally by inferior epigastric artery and • Inferiorly by inguinal ligament.
- 15. CAUSES of INGUINAL HERNIA • 1. Congenital Persistent processus vaginalis sac: chief cause of indirect hernia. • 2. Collagen fibre disorder • Smoking: Acquired collagen deficiency • 3. Obesity • 4. Chronic causes of increased intra-abdominal pressure • Chronic cough • Chronic constipation • Ascites • 5. Weakness of conjoined tendon/rupture of a few fibres • Lifting heavy weight • Post appendicectomy-injury to ilioinguinal nerve. • Chronic illness/debilitating disease causing weakness of transversalis fascia in the Hesselbach's area.
- 16. Classification of Inguinal Hernia • INDIRECT HERNIA : It comes out through internal ring along with the cord. It is lateral to the inferior Epigastric Artery. • DIRECT HERNIA : It occurs through posterior wall of Inguinal Canal through “HESSELBACH’S TRIANGLE”
- 17. INDIRECT INGUINAL HERNIA • Most common type of Hernia : 65% • More common in younger age group. • It’s bilateral in 30% cases. • Sac is thin & Neck is narrow
- 18. DIRECT INGUINAL HERNIA • 10 - 15% of Hernias are Direct. • 50% Direct Hernia occurs bilaterally. • 35% Inguinal Hernias are Direct. • Uncommon n Females & Children. • Its always acquired, due to weakening of posterior wall of Inguinal Canal. • Sac is thick with wide neck. • Occurs through Hesselbach’s Triangle.
- 20. INVESTIGATIONS Physical Examination • 1. Ask the patient to cough-expansile impulse is felt at the root of scrotum. • 2. Getting above the swelling• should be done in the standing position. • 3. Reducibility-ask the patient to lie down. If the swelling becomes smaller or disappears, it is a hernia • 4. External ring invagination test: On asking the patient to cough, the impulse touches the pulp of the finger in direct hernia and the tip in indirect hernia • 5. Internal ring occlusion test: After reducing swelling, on asking patient to cough a. If impulse and the swelling are seen, it is a direct hernia b. If the swelling is not seen, it is an indirect hernia.
- 21. INVESTIGATIONS • ULTRASOUND: To detect the contents of Hernia & its reducibility. • MRI : To know the anatomy, helpful in inflamed hernia. • Chest X-Ray : To rule out chronic bronchitis
- 22. TREATMENT • 1. Herniotomy : Excision of the sac alone is done in patients up to 14-16 years of age (children). Hernia occurs due to preformed sac. Hence, no repair is necessary.
- 23. TREATMENT • 2. Herniorrhaphy : It involves a surgeon making a long incision directly over the hernia then using surgical tools to open the cut enough to access it. Tissues or a displaced organ are then returned to their original location, and the hernia sac is removed.
- 24. TREATMENT • 3. Hernioplasty : It is the type of hernia repair surgery where a mesh patch is sewn over the weakened region of tissue
- 25. FEMORAL HERNIA • Herniation of intra-abdominal contents through the femoral canal is described as femoral hernia. • Commonly the hernia is unilateral, the right side being affected more often than the left side. • It is bilateral in about 15-20% of the patients. • Men : Women – 1 : 2
- 27. SURGICAL ANATOMY • Anatomy of Femoral Canal and Femoral Ring • The femoral canal extends from the femoral ring to the saphenous ring. It is 1.6 inches below and lateral to the pubic tubercle. It is the innermost compartment of femoral sheath. • Contents of femoral canal are Fat, Fascia & Lymphatics Femoral sheath: • Fascia transversalis make anterior layer of the femoral sheath. • Fascia iliaca : make posterior layer of the femoral sheath. • Femoral vein is in the middle compartment of the femoral sheath • Femoral artery is in the lateral compartment.
- 28. SURGICAL ANATOMY Boundaries of femoral ring • • Anterior: Inguinal ligament • • Posterior: Ligament of Cooper, iliopectineal ligament. • • Medial: Lacunar ligament (Gimbemat's ligament) • • Lateral: Thin septum which separates the femoral canal from femoral vein (silver fascia).
- 29. COURSE OF DEVELOPMENT • As the hernia comes into the femoral canal, it is an oblong swelling due to the rigid femoral canal. When it comes out through the saphenous opening, it expands and becomes retort shaped. • CAUSES: 1. Repeated Pregnancy 2. Wide Femoral Canal
- 30. TREATMENT • Low operation of Lockwood • High operation of McEvedy • Henry's approach
- 31. Umbilical Hernia • Umbilical hernia occurs when intestine, fat, or fluid pushes through a weak spot in the belly. This causes a bulge near the belly button, or navel • May be Congenital which appear in infancy or Acquired- increased in intra- abdominal pressure, commonly seen in obese or pregnant women.
- 32. TREATMENT • In 93-95 % of congenital cases it disappear after some months of birth. INDICATION OF SURGERY o If persists even after age of 2 Years o If the defect is more than 2cm in size o Acquired Umbilical Hernia
- 33. TREATMENT SURGERIES Primary closure of defect Umbilectomy Laparoscopic Repair Sublay Mesh repair : >3 cm
- 34. EPIGASTRIC HERNIA • Common in Males. • Extraperitoneal fat protrudes through a defect in the decussation of the fibers of Linea Alba. Anywhere between Xiphoid Process & Umbilicus. • It is Sacless Hernia, but later can enlarge & protrude part of peritoneum. Presenting as a true Epigastric Hernia. • Often Asymptomatic • Impulse with coughing
- 36. TREATMENT • Through a vertical incision. • Large defect is supported with preperitoneal mesh.
- 37. HERNIA SIGN & SYMPTOMS • Small to moderate size hernia don’t usually causes any symptoms. • Large hernia may be noticeable and cause same discomfort. - Pain when lifting heavy object - Tenderness - Bulging • Severe symptoms - Severe and sudden pain - Nausea - Vomiting
- 38. ABDOMINAL HERNIA PHARMACOLOGICAL MANAGEMENT 1. Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) (for patients with mild to moderate pain) i.) Ibuprofen ii.) Diclofenac 2. ANTIBIOTICS (used if the patient has strangulated hernia or before open surgeries) i) Gentamicin + Ampicillin 3. Antianxiety Agents (indicated for patients who may experience significant anxiety before a surgery) i) Lorazepam ii) Midazolam
- 39. ACUTE COMPLICATIONS • Strangulation Hernia Formation • Inflammation or Inflamed Hernia Formation • Irreducible Hernia Formation • Obstruction of any lumen, such as bowel obstruction in intestinal hernias • Hemorrhage/ Haematoma Formation • Autoimmune problems • Irreducibility
- 41. CHRONIC COMPLICATIONS • Postoperative Pain Syndrome • Hernia Recurrence • Foreign body reaction • Mesh Infection & Erosion to bladder, bowel & vessels • Wound Infection • Ischemia • Necrosis