

Recomendados
Más contenido relacionado
Destacado
Destacado (20)
Similar a Hypertension summary
Similar a Hypertension summary (20)
Más de Dr. Rubz
Más de Dr. Rubz (20)
Último
Último (20)
Hypertension summary
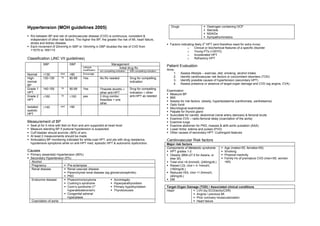
- 1. Hypertension (MOH guidelines 2005) Drugs Oestrogen containing OCP Steroids NSAIDs R/s between BP and risk of cardiovascular disease (CVD) is continuous, consistent & Sympathomimetics independent of other risk factors. The higher the BP, the greater the risk of MI, heart failure, stroke and kidney disease. o Factors indicating likely 2 HPT (and therefore need for extra invxs) Each increment of 20mmHg in SBP or 10mmHg in DBP doubles the risk of CVD from o Clinical or biochemical features of a specific disorder 115/75 to 185/115 o Young PTs (<30YO) o Accelerated HPT Classification (JNC VII guidelines) o Refractory HPT SBP DBP Management Lifestyle Patient Evaluation Initial drug Rx modification w/o compelling indication With compelling indication Aims: Normal <130 And <80 Encourage 1. Assess lifestyle – exercise, diet, smoking, alcohol intake High- 130-139 Or 80-89 Yes No Rx needed Drug for compelling 2. Identify cardiovascular risk factors or concomitant disorders (TOD) normal indication 3. Identify possible causes of hypertension (secondary HPT) BP 4. Assess presence or absence of target-organ damage and CVD (eg angina, CVA) Grade 1 140-159 Or 90-99 Yes Thiazide diuretic ± Drug for compelling Examination HPT other anti-HPT indication ± other Measure BP Grade 2 ≥160 Or ≥100 yes 2 drug combo: anti-HPT as needed BMI HPT thiazides + one Assess for risk factors: obesity, hyperlipidaemia (xanthomata, xanthelasma) other Optic fundi Isolated ≥140 and <90 Neurological examination systolic Palpate for thyroid gland HPT Auscultate for carotid, abdominal (renal artery stenosis) & femoral bruits Examine CVS – radio-femoral delay (coarctation of the aorta) Measurement of BP Examine lungs Seat pt for 5 mins with feet on floor and arm supported at heart level Examine abdomen for PKD, masses & abN aortic pulsation (AAA) Measure standing BP if postural hypotension is suspected. Lower limbs: edema and pulses (PVD) Cuff bladder should encircle ≥80% of arm. Other causes of secondary HPT: Cushingoid features At least 2 measurements should be made. Ambulatory BP monitoring indicated for white-coat HPT, and pts with drug resistance, Cardiovascular Risk factors hypotensive symptoms while on anti-HPT med, episodic HPT & autonomic dysfunction. Major risk factors Components of Metabolic syndrome Age (males>55, females>65) Causes HPT grades 1-2 Smoking Primary (essential) Hypertension (95%) Obesity (BMI≥27.5 for Asians, or Physical inactivity Secondary Hypertension (5%) else 30) Family Hx of premature CVD (men<55, women Alcohol Total chol >6.2mmol/L (240mg/dL) <65) Pregnancy Pre-eclampsia Raised LDL chol > 4.1mmol/L Renal disease Renal vascular disease (160mg/dL) Parenchymal renal disease (eg glomerulonephritis) Reduced HDL chol <1.0mmol/L PKD (40mg/dL) Endocrine disease Phaeochromocytoma Acromegaly DM Cushing’s syndrome Hyperparathyroidism o Conn’s syndrome (1 Primary hypothyroidism Target-Organ Damage (TOD) / Associated clinical conditions hyperaldosteronism) Thyrotoxicosis Heart LVH (by ECG/echo/CXR) Congenital adrenal Angina / previous MI hyperplasia Prior coronary revascularization Coarctation of aorta Heart failure
- 2. Brain Ischemic Stroke Treatment Cerebral hemorrhage Aim: reduce cardiovascular and renal morbidity and mortality TIA Target: <140/90mmHg; Hypertensive encephalopathy – HPT, neuro deficits, papilloedema. <130/80mmHg for DM or chronic renal disease Reversible if HPT is controlled at least high-normal (<140/90mmHg) for elderly, provided no orthostatic hypotension Renal Proteinuria >0.5g/24h occurs Microalbuminaemia (albumin:creatinine ratio >30mg/g) renal impairment (plasma creatinine concentration >132 mmol/L) Diabetic nephropathy Algorithm for Rx of HPT Lifestyle modification Retinopathy Grade 1: arteriolar thickening, tortuosity, silver wiring Grade 2: Grade 1 + arteriovenous nipping Grade 3: Grade 2 + flame or blot hemorrhages & cotton wool exudates Target BP not achieved Grade 4: Grade 3 + papilloedema Atherosclerosis U/S or radiological evidence of atherosclerotic plaques (carotids, iliac, femoral & peripheral arteries, aorta) Initial drug choices Vascular Dissecting aneurysm Symptomatic arterial disease Malignant HPT Accelerated microvascular damage with necrosis in the walls of small HPT w/o compelling HPT w compelling arteries and arterioles. indications indications Intravascular thrombosis Dx: HPT + rapidly progressive end-organ damage (retinopathy, renal failure, HPT encephalopathy) Stage 1 HPT Stage 2 HPT Use drug for L. ventricular failure may result. Poor Px if untreated. Thiazide diuretic for 2 drug combination compelling reason most for most (usually Add diuretics, ACEI, Consider adding thiazide diuretic + ARB, β-blocker and Investigations ACEI, ARB, β-blocker ACEI, ARB, β-blocker CCB as needed Routine Investigations or CCB if target not or CCB) ECG Left ventricular hypertrophy achieved Coronary artery disease FBC Haematocrit + U/E/Cr S. potassium – hypoK alkalosis may indicate Conn’s syndrome Follow-up & Monitoring Creatinine for GFR estimation Monthly f/u until BP goal is Calcium reached. 3 to 6 mthly f/u thereafter. Urinalysis Blood, protein & glucose S. potassium & creatinine Fasting lipids monitoring 1-2X per year Blood glucose Additional investigation if indicated CXR Cardiomegaly Heart failure Coarctation of aorta 1) Lifestyle modification Ambulatory BP recording White-coat HPT Diet: moderation of alcohol consumption, low sodium diet, lower intake of chol and Borderline HPT saturated fats ± Rx of hyperlipidaemia, maintenance of adequate intake of dietary K 2D echo Detect & quantify LVH Weight reduction, increased physical activity Renal U/S Renal disease Smoking cessation Renal angiography Renal artery stenosis Urinary catecholamines Phaeochromocytoma Urinary cortisol & Assessment of Cushing’s syndrome dexamethasone suppression test Plasma renin activity & Detect primary hyperaldosteronism (Conn’s syndrome) aldosterone
- 3. 2) Pharmacological Rx Pharmacological Rx in pregnancy Drug choice for compelling indications Use methyldopa, β-blockers & vasodilators. th Diuretic β-blocker ACE-I ARB CCB Aldosterone Monitor for devt of pre-eclampsia after 20 wk of gestation (new onset/worsening HPT, antagonist albuminuria, hyperuricaemia, coagulation abNs) Heart failure X XX XX X X Post-MI X X X Management of Hypertensive Emergencies High coronary dz X X X X Do not lower BP too quickly – may compromise tissue perfusion risk With acute TOD: hospitalize, parenteral drug therapy (labetalol, nitroglycerin, hydralazine, Diabetes X X *X *X X Na nitroprusside) Chronic renal dz X X Without acute TOD: immediate combination PO anti-HPT Rx, monitoring for TOD. Recurrent stroke X X prevention** *ACE-I & ARB based Rx slow progression of diabetic & non-diabetic nephropathy **Add anti-platelet agents (eg aspirin, ticlopidine, clopidogrel) Drug Absolute CI / use with Side Effects caution Hypertensive Emergencies Diuretic Gout Hyperuricaemia (chlorothiazide, Hx of hypoNa + Impotence Definitions: hydrochlorothiazide) Dyslipidaemia Glucose intolerance Hypertensive crisis – no definite BP level used to define a hypertensive crisis. DBP of β-blocker Asthma Raise concentration of 120-130 mmHg used as a guide. Includes: – (atenolol, COPD cholesterol o Hypertensive emergency – elevated BP a/w acute or ongoing end-organ propanolol) Heart block Aggravate asthma, HF, PVD dysfunction or damage Dyslipidaemia o Hypertensive urgency – elevated BP a/w imminent end-organ Athletes / physically active dysfunction or damage PTs Peripheral vascular disease Types of Hypertensive emergencies ACE-I Pregnancy First dose hypotension 1. Hypertensive encephalopathy – need to d/dx from stroke, as reduction of BP is (Captopril) Bilat renal art stenosis + Cough contraindicated in stroke. BP is significantly ↑ in HPT encephalopathy, but only mildly ↑ HyperK Rash in stroke Proteinuria 2. Acute pulmonary oedema (Hypertensive left ventricular failure) – due to Hyper K+ decompensation secondary to excessive afterload Renal dysfunction 3. Acute aortic dissection – new AR murmur may be heard Unpleasant metallic taste 4. AMI / acute coronary syndrome – due to increased myocardial O2 demand *monitor U/E/Cr before and 5. Haemorrhagic/ischaemic stroke or SAH after starting Rx 6. Acute renal failure ARB Pregnancy *does not cause cough c.f 7. Eclampsia / preeclampsia (losartan) Bilat renal art stenosis ACEI 8. Phaechromocytoma crises + HyperK 9. Recreational drugs (eg ectasy) CCB Heart block Flushing (nifidepine, CCF Palpitation Types of Hypertensive urgencies amlodipine, Fluid retention 1. Elevated BP with retinal changes diltiazem) Bradycardia (for diltiazem & 2. CRF verapamil) 3. Preeclampsia + Aldosterone May cause hyperK : avoid in + antagonist Pts with K >5.0 mEq/L while (Spironolactone) not on med
- 4. Management o Use with phentolamine for catecholamine crises A) Initial Mx Dose: IV 1mg boluses & titrate Stabilize ABC Esmolol Indications: aortic dissection Low flow supplemental O2 Dose: IV 250-500μg/kg/min for 1 min, then 50-100μg/kg/min for 4mins. Monitor Repeat as required. ECG Phentolamine Indications: Use with phentolamine for catecholamine crises Pulse oximetry Dose: IV 5-15mg Vital signs q5-10 mins Hydralazine Indications: Rx of choice for predelivery eclampsia Check BP Manual BP taking Dose: IV 5-10mg boluses q15min & titrate Use correct cuff size Disposition – admit ICU Check other arm Recheck later D/dx btwn HPT Clinical exam B2) Mx of HPT Urgencies (ie end-organ dysfunction imminent) emergency & urgency – Fundoscopy – haemorrhage, exudates, papilloedema o Target – Lower BP over 24-48 hrs to DBP of 100mmHg look for signs of end- Neuro exam – AMS, focal neuro deficits Felodipine Dose: organ damage CVS exam – LVFailure, AR murmur (aortic dissectn) o >65YO: 2.5mg PO Bedside tests o <65YO: 5.0mg PO, then 5.0mg bd ECG Captopril Dose: 25.0mg stat, then bd or tds Urine dipstick – haematuria & proteinuria for renal dz Disposition Responsive to Rx & BP acceptable after 4 hrs of monitoring – UPT – eclampsia, preeclampsia discharge with F/U w/in 48 hrs Lab invx FBC Newly dxed HPT with uncertain cause – admit to Gen Med for U/E/Cr evaluation of secondary causes of HPT Cardiac enzymes & Troponin T CXR – LV failure, widened mediastinum Summary of Drugs used in Hypertensive Crises CT head – if AMS or stroke suspected (IMPT: rule out stroke before Drug Dose Special indications Others lowering BP!) HPT Emergencies CT thorax – if aortic dissection suspected Na Nitroprusside IV 0.25μ/kg/min All except eclampsia SE: Thiocynate / cyanide toxicity B1) Mx of HPT Emergencies (ie end-organ dysfunction present) Labetalol IV 25-50 mg bolus IHD CI: asthma, Target Followed by 25-50 mg q5-10 Aortic dissection COLD, CCF, o Lower MAP to by 20-25% or DBP to no less than 100 mmHg within a few hrs o Then aim for 160/100 mmHg over the next 2-6 hrs mins ↓HR, heartblk Nitroglycerine IV 5-100μg/min Unstable angina Na Indication: all HPT emergencies except predelivery eclampsia nitroprusside Dose: IV 0.25μ/kg/min, titrate to response. (Max 10μg/kg/min for only Propanolol IV 1mg boluses Thoracic aortic dissect (Prop. + nitroprus) 10mins) Catecholamine crises (Prop. + phentol.) SE: cyanide & thiocynate toxicity after prolonged used – lactic acidosis, Esmolol IV 250-500μg/kg/min for 1 min, Aortic dissection AMS, clinical deterioration. Therefore monitor closely if used then 50-100μg/kg/min for 4mins Labetalol Indications: failure of nitroprusside. Good for IHD (↓HR & O2 demand) Phentolamine IV 5-15mg Catecholamine crises (Prop. + Phentol.) & aortic dissection (↓ systolic ejection force & shear stress) Hydralazine IV 5-10mg boluses q15min Eclampsia CI: asthma, COLD, CCF, bradycardia, heart block HPT Urgencies Dose: Felodipine >65YO: 2.5mg PO o IV 25-50 mg bolus, <65YO: 5.0mg PO, then 5.0mg o followed by 25-50 mg q5-10 mins (max 300mg) OR infusion rate bd 0.5-2.0 mg/min Captopril 25.0mg stat, then bd or tds Nitroglycerine Indications: HPT complicating unstable angina Dose: IV 5-100μg/min, titrate to response SE: headache, vomiting Digitally signed by DR WANA HLA SHWE DN: cn=DR WANA HLA SHWE, c=MY, o=UCSI Propanolol Indications: University, School of Medicine, KT-Campus, Terengganu, ou=Internal Medicine Group, o Use with nitroprusside for thoracic aortic dissection email=wunna.hlashwe@gmail.com Reason: This document is for UCSI year 4 students. Date: 2009.02.24 10:08:40 +08'00'