Bohomolets Microbiology Lesson #5
•Download as DOC, PDF•
2 likes•1,142 views

By Ms. Kostiuk from Microbiology department

Recommended
Recommended
More Related Content
What's hot
What's hot (19)
Viewers also liked
Similar to Bohomolets Microbiology Lesson #5
Similar to Bohomolets Microbiology Lesson #5 (20)
More from Dr. Rubz
More from Dr. Rubz (20)
Recently uploaded
Recently uploaded (20)
Bohomolets Microbiology Lesson #5
- 1. Lesson N5: LABORATORY DIAGNOSIS OF ENTERIC FEVER 1.Scientifically methodical ground of theme The term enteric fever includes typhoid fever caused by S.typhi and paratyphoid fever caused by S. paratyphi A, B and C. In developing countries S.typhi is commonly isolated by laboratories but date are incompletily. It has been estimated that between 10 and 500 cases of typhoid per100 000 of the population occur annually throughout the developing world. 2.Educational purpose Students must know: 1. Structure, staining properties and cultivation of S. typhi. S. paratyphi A, S. schottmuelleri. 2. Antigenic structure of S. typhi. S. paratyphi A, S. schottmuelleri. 3. Fermentative properties of S. typhi. S. paratyphi A, S. schottmuelleri. 4. Epidemiology and pathogenesis of typhoid fever and paratyphoids. 5. Methods of laboratory diagnosis of diseases, main methods of prophylaxis and treatment. Students should be able to: – prepare the smears from tested material; – stain the smears by Gram’s technique; – make microscopical examination of the smears; – value the growth of Salmonellae in Rapoport’s media; – the biochemical properties of Salmonellae according to Hiss’media. – value Widal reaction; – value IHAT to diagnosis typhoid fever carring 3.Chart of topic content. Enteric Fever and Paratyphoid Salmonellae. The causative agent of typhoid fever, Salmonella typhi,was discovered in 1880 by K. Eberth and isolated in pure culture in 1884 by G. Gaffky.It causative role was conformed by Metchnikoff and Bezredka(1900) In 1896 the French scientists C. Archard and R. Bensaude isolated S. paratyphi B from urine and pus collected from patients with clinical symptoms of typhoid fever. Salmonella paratyphi A was isolated by Gwyn in 1898 .The causative agent of paratyphoid B (Salmonella schottmuelleri) was studied in 1900 by H. Schottmueller. Morphology. The morphology of the typhoid salmonella corresponds to the general characteristics of the Enterobacteriaceae family. The paratyphoid salmonellae do not differ from the typhoid organisms in shape, size, type of flagella, and staining properties. Cultivation. The typhoid and paratyphoid organisms are facultative anaerobes. The optimum temperature for growth is 37° C, but they also grow at temperatures between 15 and 41°C. They grow on ordinary media at pH 6.8-7.2. On meat-peptone agar S. typhi forms semitransparent colonies which are half or one-third the size of E. coli colonies.Cultures on agar slants form a moist transparent film of growth without a pigment and in meat broth they produce a uniform turbidity. On Ploskirev's and Endo's media S. typhi and S. paratyphi form semitransparent, colourless or pale-pink coloured colonies. On Levin's medium containing eosin and methylene blue the colonies are transparent and bluish in colour and on bismuth-sulphite agar they are glistening and black. The colonies produced by S. paratyphi A on nutrient media (Ploskirev's, Endo's, etc.) are similar to those of S. typhi . Colonies of S. schottmuelleri have a rougher appearance and after they have been incubated for 24 hours and then left at room temperature for several days, mucous swellings appear at their edges. This is a characteristic differential cultural property. Fermentative properties. S. typhi does not liquefy gelatin, nor does it produce indole. It produces hydrogen sulphide, and reduces nitrates to nitrites. The organisms do not coagulate milk, but they give rise to a slightly pink colouration in litmus milk and cause no changes in Rotberger's medium. They ferment glucose, mannitol, maltose, levulose, galactose, raffinose, dextrin, glycerin, sorbitol and, sometimes, xylose, with acid formation. S. paratyphi ferments carbohydrates, with acid and gas formation, and is also distinguished by other properties.Two types of S. typhi occur in nature: xylose-positive and xylose-negative. They possess lysin decarboxylase, ornithine decarboxylase and oxidase activity. In the process of dissociation S. typhi changes from the S-form to the R-form. This variation is associated with loss of the somatic 0-antigen (which is of most immunogenic value) and, quite frequently, with loss of the Vi- antigen. 1
- 2. Toxin production. S. typhi contains gluco-lipo-protein complexes. The endotoxin is obtained by extracting the bacterial emulsion with trichloracetic acid. This endotoxin is thermostable, surviving a temperature of 120° C for 30 minutes, and is characterized by a highly specific precipitin reaction and pronounced toxic and antigenic properties. Antigenic structure. S. typhi possesses a flagellar H-antigen and thermostable somatic 0- and Vi- antigens. All three antigens give rise to the production of specific antibodies in the body, i. e. H-, 0-, and Vi- agglutinins. H-agglutinins bring about a large-flocculent agglutination, while 0- and Vi-agglutinins produce fine- granular agglutination. The antigens differ in their sensitivity to chemical substances. The O-antigen is destroyed by formalin but is unaffected by exposure to weak phenol solutions. The H-antigen, on the contrary, withstands formalin but is destroyed by phenol. S. typhi, grown on agar containing phenol in a ratio of 1:1000, loses the H-antigen after several subcultures. This antigen is also destroyed on exposure to alcohol. These methods are employed to obtain the 0-antigen in its pure form. The H-antigen is isolated by treating the bacterial emulsion with formalin or by using a broth culture which contains a large number of flagellar components. Immunization with H-and 0-antigens is employed for obtaining the corresponding agglutinating sera. The discovery of the Vi-antigen isolated from virulent S. typhi is of great theoretical interest and practical importance.Felix and Pitt, who first described this antigen, believed that it was related to virulence and gave it name “Vi antigen”. It is analogous to the K antigens of coliforms. It is heat labile. Many strains fail to agglutinate with the O antiserum when freshly isolated. This is due to presence of Vi antigen. It is related to mouse virulence as judged by the production of lethal infection by intraperitoneal inoculation but its role in natural human disease is not known. The Vi antibody dissapeares early in convalescence. Its presence indicates the developmant of carrier state. Classification. The salmonellae of enteric fever together with the causative agents of toxinfections have been included in the genus Salmonella (named after the bacteriologist D. Salmon) on the basis of their antigenic structure and other properties. At present, about 2000 species and types of this genus are known. F. Kauffmann and P. White classified the typhoid-paratyphoid salmonellae into a number of groups according to antigenic structure and determined 65 somatic 0-antigens. For instance, S. typhi (group D) contains three different 0-antigens — 9, 12, and Vi .S. paratyphi A alone constitutes group A, and S. schottmuelleri belongs to group B. It has been proved by F. Andrewes that the flagellar H-antigen is not homogeneous but is composed of two phases: phase 1 is specific and agglutinable by specific serum, phase 2 is non-specific and agglutinable not only by specific, but also by group sera. Salmonellae, which possess two-phase H-antigens, are known as diphasic, while those which possess only the specific H-antigen are monophasic. Resistance. Typhoid and paratyphoid A and B salmonellae survive in ice for several months, in soil contaminated with faeces and urine of patients and carriers for up to 3 months, in butter, cheese, meat and bread for 1-3 months, in soil, faecal masses, and water for several weeks, and in vegetables and fruits for 5-10 days. They remain unaffected by desiccation and live for a long time in dry faeces. Salmonellae survive for only a short time (3-5 days) in polluted water owing to the presence of a large number of saprophytic microbes and substances harmful to pathogenic microorganisms. S. paratyphi A are susceptible to heat and are destroyed at 56° C in 45-60 minutes, and when exposed to the usual disinfectant solutions of phenol, calcium chloride, and chloramine, perish in several minutes. The presence of active chlorine in water in a dose of 0.5-1 mg per litre provides reliable protection from S. typhi and S. paratyphi A. Pathogenicity for animals. Animals do not naturally acquire typhoid fever and paratyphoids. Therefore, these diseases are anthroponoses. Pathogenesis and diseases in man. The causative agent is primarily located in the intestinal tract. Infection takes place through the mouth (digestive stage). Cyclic recurrences and development of certain pathophysiological changes characterize the pathogenesis of typhoid fever and paratyphoids. There is a certain time interval after the salmonellae penetrate into the intestine, during which inflammatory processes develop in the isolated follicles and Peyer's patches of the lower region of the small intestine (invasive stage). As a result of deterioration of the defence mechanism of the lymphatic apparatus in the small intestine the organisms enter the blood (bacteriemia stage). Here they are partially destroyed by the bactericidal substances contained in the blood, with endotoxin formation. During bacteraemia typhoid salmonellae invade the patient's body, penetrating into the lymph nodes, spleen, bone marrow, liver, and other organs (parenchymal diffusion stage). This period coincides with the early symptoms of the disease and lasts for a week. During the second week of the disease endotoxins accumulate in Peyer's patches, are absorbed by the blood, and cause intoxication. The general clinical picture of the disease is characterized by status typhosus, disturbances of thermoregulation, activity of the central and vegetative nervous systems, cardiovascular activity, etc. 2
- 3. On the third week of the disease a large number of typhoid bacteria enter the intestine from the bile ducts and Lieberkuhn's glands. Some of these bacteria are excreted in the faeces, while others reenter the Peyer's patches and solitary follicles, which had been previously sensitized by the salmonellae in the initial stage. This results in the development of hyperergia and ulcerative processes. Lesions are most pronounced in Peyer's patches and solitary follicles and may be followed by perforation of the intestine and peritonitis (excretory and allergic stage). The typhoid-paratyphoid salmonellae together with products of their metabolism induce antibody production and promote phagocytosis. These processes reach their peak on the fifth-sixth week of the disease and eventually lead to recovery from the disease. Clinical recovery (recovery stage) does not coincide with the elimination of the pathogenic bacteria from the body. The majority of convalescents become carriers during the first weeks following recovery, and 3-5 per cent of the cases continue to excrete the organisms for many months and years after the attack and, sometimes, for life. Inflammatory processes in the gall bladder (cholecystitis) and liver are the main causes of a carrier state since these organs serve as favourable media for the bacteria, where the latter multiply and live for long periods. Besides this, typhoid-paratyphoid salmonellae may affect the kidneys and urinary bladder, giving rise to pyelitis and cystitis. In such lesions the organisms are excreted in the urine. In one, two, or three weeks following marked improvement in the patient's condition, relapses may occur as a result of reduced immunobiological activity of the human body and hence a low-grade immunity is produced. Due to the wide range in the severity of typhoid fever from gravely fatal cases to mild ambulant forms it cannot be differentiated from paratyphoids and other infections by clinical symptoms. Laboratory diagnosis of these diseases is of decisive importance. In recent years typhoid fever has changed from an epidemic to a sporadic infection, being milder in nature and rarely producing complications Diseases caused by S. paratyphi are similar to typhoid fever. The period of incubation and duration of the disease are somewhat shorter in paratyphoid infections than in typhoid fever. Immunity. Immunity acquired after typhoid fever and paratyphoids is relatively stable but relapses and reinfections sometimes occur. Antibiotics, used as therapeutic agents, inhibit the immunogenic activity of the pathogens, which change rapidly and lose their O- and Vi-antigens. Laboratory diagnosis. The present laboratory diagnosis of typhoid fever and paratyphoids is based on the pathogenesis of these diseases. 1. Isolation of haemoculture. Bacteraemia appears during the first days of the infection. Thus, for culture isolation 10-15 ml of blood (15-20 ml during the second week of the disease and 30-40 ml during the third week) are inoculated into 100, 150 and 200 ml of 10 per cent bile broth, after which cultures are incubated at 37° C and on the second day subcultured onto one of the differential media (Ploskirev's, Endo's, Levin’s) or common meat- peptone agar. The isolated culture is identified by inoculation into a series of differential media and by the agglutination reaction. The latter is performed by the glass-slide method using monoreceptor sera or by the test-tube method using purified specific sera. 2. Serological method. Sufficient number of agglutinins accumulate in the blood on the second week of the disease, and they are detected by the Widal reaction. Diagnostic typhoid and paratyphoid A and B suspensions are employed in this reaction. The fact that individuals treated with antibiotics may yield a low titre reaction must be taken into consideration. The reaction is valued positive in patient's serum in dilution 1 : 200 and higher. The Widal reaction may be positive not only in patients but also in those who had suffered the disease in the past and in vaccinated individuals. For this reason diagnostic suspensions of O- and H-antigens are employed in this reaction. The sera of vaccinated people and convalescents contain H-agglutinins for a long time, while the sera of patients contain O-agglutinins at the height of the disease. In typhoid fever and paratyphoids the agglutination reaction may sometimes be of a group character since the patient's serum contains agglutinins not only to specific but also to group antigens which occur in other bacteria. In such cases the patient's blood must be sampled again in 5-6 days and the Widal reaction repeated. Increase of the agglutinin titre makes laboratory diagnosis easier. In cases when the serum titre shows an equal rise with several antigens, 0-, H-, and Vi-agglutinins are detected separately. The Vi-agglutination reaction is employed for identification of S. typhi carriers. This reaction is performed with sera (inactivated at 56° C for 30 minutes and diluted in the ratio of 1:10-1:80) and diagnostic Vi-suspensions. Individuals who give a positive Vi-agglutination reaction are subjected to microbiological examination for isolation of S. typhi from the bile, faeces, and urine. The best results are obtained when Vi-haemagglutination is employed. For quick serological diagnosis of typhoid fever and paratyphoids Nobel's agglutination method and agglutination on glass by the Minkevitch-Brumpt method are carried out. In the latter case the bacterial emulsion is agglutinated in a drop of undiluted blood placed on a slide. 3
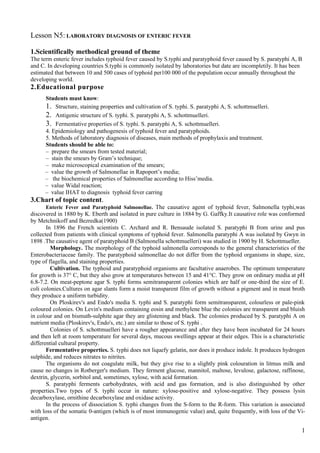
- 4. 3. A pure culture is isolated from faeces and urine during the first, second, and third weeks of the disease. The test material is inoculated into bile broth, Muller's medium, Ploskirev's medium, or bismuth sulphite agar. Isolation and identification of the pure culture are performed in the same way as in blood examination. Selective media are recommended for isolation of the typhoid-paratyphoid organisms from water, sewage, milk, and faeces of healthy individuals. These media slightly inhibit the growth of pathogenic strains of typhoid- paratyphoid organisms and greatly suppress the-growth of saprophytic microflora. A reaction for the detection of a rise in the phage titre is employed in typhoid fever and paratyphoid diagnosis. This reaction is based on the fact that the specific (indicator) phage multiplies only when it is in contact with homologous salmonellae. An increase in the number of phage corpuscles in the test tube as compared to the control tube is indicative of the presence of organisms homologous to the phage used. This reaction is highly sensitive and specific and permits to reveal the presence of the salmonellae in various substrates in 11-22 hours without the necessity of isolating the organisms in a pure culture. The reaction is valued positive if the increase in the number of corpuscles in the tube containing the test specimen is not less than 5-10 times that in the control tube. When unagglutinable cultures of the typhoid and paratyphoid organisms are isolated, the agglutination reaction is performed using Vi-sera. If the latter are not available, the tested culture is heated for 30 minutes at 60° C or for 5 minutes at 100° C. The agglutination reaction is carried out with a suspension of this heated culture. In some cases a bacteriological examination of duodenal juice (in search for carriers), bone marrow, and material obtained from roseolas is conducted. Phage typing of typho-paratyphoid organisms is sometimes employed. The isolated culture is identified by type-specific O- and Vi-phages. Sources of typhoid and paratyphoid infections are revealed by this method. Water is examined for the presence of typho-paratyphoid bacteria by filtering large volumes (2-3 litres) through membrane filters and subsequent inoculation on plates containing bismuth sulphite agar. If the organisms are present, they produce black colonies in 24-48 hours. The reaction of increase in phage titre is carried out simultaneously. 100% 80% А-Widal aggluitinati 60% on В-Feces culture 40% С-blood 20% culture 0% 1 2 3 4 5 Figure N1: Laboratory diagnosis of typhoid fever. The approximate percentages of tests found positive during different stages of disease (from 1st to 5th week). Treatment. Patients with typhoid fever and paratyphoids are prescribed chloramphenicol, oxytetracycline, and nitrofuran preparations. These drugs markedly decrease the severity of the disease and diminish its duration. Great importance is assigned to general non-specific treatment (dietetic and symptomatic). Treatment must be applied until complete clinical recovery is achieved, and should never be discontinued as soon as the bacteria disappear from the blood, urine, and faeces since this may lead to a relapse. Mortality has now fallen to 0.2-0.5 per cent (in 1913 it was 25 per cent). The eradication of the organisms from salmonellae carriers is a very difficult problem. Prophylaxis. General measures amount to rendering harmless the sources of infection. This is achieved by timely diagnosis, hospitalization of patients, disinfection of the sources, and identification and treatment of carriers. Of great importance in prevention of typhoid fever and paratyphoids are such measures as disinfection of water, safeguarding water supplies from pollution, systematic and thorough cleaning of inhabited areas, fly control, and 4
- 5. protection of foodstuff's and water from flies. Washing of hands before meals and after using the toilet is necessary. Regular examination of personnel in food-processing factories for identification of carriers is also extremely important. In the presence of epidemiological indications specific prophylaxis of typhoid infections is accomplished by vaccination. Several varieties of vaccines are prepared: typhoid vaccine (monovaccine), typhoid and paratyphoid B vaccine (divaccine). Good effects are obtained also with a chemical associated adsorbed vaccine which contains 0- and Vi- antigens of typhoid, paratyphoid B, and a concentrated purified and sorbed tetanus anatoxin. All antigens included in the vaccine are adsorbed on aluminium hydroxide. A new areactogenic vaccine consisting of the Vi-antigen of typhoid fever Salmonella organisms has been produced. It is marked by high efficacy and is used in immunization of adults and children under seven years of age. When there are epidemiological indications, all the above-mentioned vaccines are used according to instructions and special directions of the sanitary and epidemiological service. 4. Student’s independent study program 1. Structure, staining properties of causative agents of enteric fever and paratyphoids. Cultivation. 2. Biochemical properties of enteric fever and paratyphoids. Fill in the table Table 1 Fermentation of Production of Microbe Glu- Mal- Man- Lac- Saccha- H2S Indole cose tose nite tose rose S. typhi S. paratyphi A S. schottmuelleri 3. Antigenic structure of salmonellae. Principles of Kauffman– White classification of Salmonellae according their antigenic structure. Practical value of Kauffman– White classification 4. Phagovars of Salmonellae. Practical value of their examination. 5. Toxin production of Salmonella 6. Make scheme, which shows epidemiology and pathogenesis of enteric fever: a – source of infectious agents (reservoir); b – mechanism of transmission ; c – factors of transmission ; d – stages of pathogenesis. 7. Main stages of isolation of bacteria from blood (hemoculture), faeces (coproculture), and from urine. 8. Serological methods of diagnosis and their practical value (Widal agglutination test, indirect haemagglutination test; indirect Vі-hemagglutination test. 9. Epidemiological value of a S. typhi carriage and its laboratory diagnosis. 10. Prophylaxis of enteric fever and paratyphoids (revealing of a source of infectious agents, pathes of transmission, factors of transmission). Specific prophylaxis. 5. Students’ practical activities: 1. To study under microscope morphology of causing agents of a typhoid fever and paratyphoids. 2. To study the peculiarities of S. typhi. S.paratyphi A, S. schottmuelleri on MPA, Endo’s, Levin’s, Ploskirev’s media etc., and in MPB. 3. To evaluate Widal reaction with patient’serum and make up conclusion. In serological diagnosis Widal's reaction is employed. Antibodies to the causative agents of typhoid, paratyphoid A and paratyphoid B fevers can be recovered in the patient's blood serum beginning from the 8th-10th day of the disease. To perform the Widal test (Table 2), draw 2-3 ml of blood from a vein or 1 ml of blood from a finger or an ear lobe and obtain serum. Successively dilute the serum in three parallel rows of test. tubes from 1:100 to 1:1600 and introduce 0-diagnosticums (usual or erythrocyte ones) of Salmonella typhi into test tubes of the first row, of Salmonella paratyphi A into test tubes of the second row, and of Salmonella paratyphi B into test tubes of the third row. The use of 0-diagnosticums makes it possible to reveal 0-antibodies which appear in the blood during the second week of the disease and disappear by the end of the illness. The diagnostic titre of antibodies in the Widal test in non-immunized subjects is 1:100 and higher. 5
- 6. Table 2 Schematic Description of the Widal Reaction Number of test the tubes Ingredient 1 2 3 4 5 6 7 Isotonic sodium – 1,0 1,0 1,0 1,0 – 1,0 chloride solution, ml Patient's serum in1:100 dilution, 1,0 1,0 → → ↑ 1,0 – ml Diagnosticum, 1,0 1,0 1,0 1,0 1,0 1,0 – drops Serum dilution 1:100 1:200 1:400 1:800 1:1600 1:100 – obtained Results Demonstration of the H-antibodies is of no diagnostic value since they are detected during convalescence, and also in vaccinated individuals and those with a history of the disease. In some cases O-antibodies may be recovered in vaccinated persons. Hence, it is necessary that the Widal test be performed over time to look for an increase in its titre. If the patient's blood serum agglutinates two or three types of diagnosticums simultaneously, the titre of agglutination should be taken into account. Typically, the specific agglutination occurs at larger and the group one at lower serum dilutions. Currently, the onset of antibiotic treatment at early stages of the disease poses difficulty in evaluating the results of the agglutination reaction since the antibody titre in patients is small and cannot be considered diagnostically significant. 4. To make conclusion according demonstration IHAT. The indirect haemagglutination test with erythrocyte monoreceptor diagnosticums O9, O12, and Vi is a more sensitive test, yielding-positive results in a greater number of cases. Antibodies to the 0-an-tigens are detected beginning from the second week of the disease. Antibodies to the Vi-antigens are recovered at later stages. Vi-anti- bodies occur most commonly in carriers of Salmonella typhi. To identify bacteria carriers, indirect haemagglutination with demonstration of antibodies belonging to Immunoglobulins G is employed (a signal method). 5. To streak patient’s feces onto Ploskirev’s medium. Termostat, t=370C for 24-48 haurs Ploskirev’s medium Speсimen (patient’s feces) 6. To familiarize with peculiarities of carbohydrates fermentation on Hiss’ media of S. typhi, S. paratyphiA, S. paratyphi B. 6. Control questions and tests Select the correct answers. 1. Salmonellae have such properties: a – inmotile; b – peritrichates; c – gram-negative; d – gram-positive; e – have capsules. 6
- 7. 2. Cultivation of Salmonellae: a – on Endo’s, Levin’s media form semitransparent, colourless colonies; b – on Endo’s and Levin’s media form red colonies; e – colonies of S. schottmuelleri are differ from S paratyphi A colonies. 3. Biochemical properties of Salmonellae: a – do not ferment a lactose and saccharose; b – S. paratyphі A produce H2S; c – according fermentation of carbohydrates S. typhі does not differ from causative agents of paratyphoids; e –salmonellae fererment all carbohydrates of Hiss’ media with the exception of saccharose. 4. Antigenic structure of Salmonellae: a – according to O-antigen they are subdivided into serological groups; b – K-antigen is determined a group of Salmonallae; c – according to Н–antigen they are subdivided into serovars; d – Vі-antigen promotes O- agglutination; e – they have no Р-antigen. 5. A source of infection is: a – sick men and animals; b – sick persons; c – bacterium carrier; d – domestic animals; e – infected foodstuff, water. 6. Typhoid fever is characterised by: a –incubation period – 1-2 hours; b – bacteriemia; c – septicemia; d – presence of an excretory- allergic period; e – penetration of disease agents into Peyer’s patches. 7. Choose the letters (a, b, c, .. etc) according the sequence of using these methods of diagnosis: a – salmonellae isolation from feces; b – salmonellae isolation from bile; c – salmonellae isolation from blood (hemoculture); d – serological method; e – salmonellae isolation from urine. Select the correct statement: 8. A – blood is inoculated onto Endo’s medium; b – feces are inoculated onto Mueller’s medium; c – blood is inoculated into Rapoport’s medium; d – feces are inoculated into Rapoport’s medium; e – urine is inoculated into bile broth. 9. A – phagotyping allows to identify a source of Salmonellae; b – O-antibodies find in the height of disease; c – Н–antibodies are characterised for bacteria carriers; d – Н-antibodies are found in vaccinated persons and in pesons which had been ill; e – O- and Н-antibodies are found in Serum in thirds period of pathogenesis. 10. The Salmonella typhi carriage can be revealed by: a – inoculation of the blood into Rapoport’s medium; b – inoculation of the feces onto plates with Mueller’s and Ploskirev’s media; c – by finding of Vі-hemagglutinins; d –finding of O-agglutinins; e –inoculation of the bile onto Endo’s medium. 7. List of literature: 1. I. S. Gaidash, V.V. Flegontova, Microbiology, virology and immunology, Lugansk, 2004, p.187-189, 213. 7