

Recomendados
Recomendados
Más contenido relacionado
Destacado
Destacado (20)
Similar a Approach to ST elevation in ECG sumary
Similar a Approach to ST elevation in ECG sumary (20)
Más de Dr. Rubz
Más de Dr. Rubz (20)
Approach to ST elevation in ECG sumary
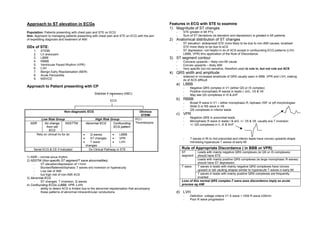
- 1. Approach to ST elevation in ECGs Features in ECG with STE to examine 1) Magnitude of ST changes Population: Patients presenting with chest pain and STE on ECG - STE greater in MI PTs Aim: Approach to managing patients presenting with chest pain and STE on ECG with the aim - Sum of ST deviations (ie elevation and depression) is greated in MI patients of expediting diagnosis and treatment of AMI 2) Anatomical distribution of ST changes - ST elevation: widespread STE more likely to be due to non-AMI causes, localised DDx of STE: STE more likely to be due to aCS 1. STEMI - ST depression: not helpful in dx of ACS except in confounding ECG patterns (LVH, 2. LV aneurysm LBBB, VPR) thru application of the Rule of Discordance 3. LBBB 3) ST segment contour 4. RBBB - Concave upwards – likely non-MI cause 5. Ventricular Paced Rhythm (VPR) - Convex upwards – likely AMI 6. LVH - Very specific but not sensitive, therefore used to rule in, but not rule out ACS 7. Benign Early Repolarisation (BER) 4) QRS width and amplitude 8. Acute Pericarditis - widened or increased amplitude of QRS usually seen in BBB, VPR and LVH, making 9. NSIVCD dx of ACS difficult a) LBBB Approach to Patient presenting with CP - Negative QRS complex in V1 (either QS or rS complex) - Positive monophasic R waves in leads I, aVL, V5 & V6 Stabilise if necessary (ABC) - May see QS complexes in III & aVF ECG b) RBBB - Broad R wave in V1 – either monophasic R, biphasic rSR’ or qR morphologies - Wide S or RS wave in V6 - QS complexes in inferior leads Non-diagnostic ECG Obvious STEMI c) VPR - Negative QRS in precordial leads Low Risk Group High Risk Group PCI / - Monophasic R wave in leads I & aVL +/- V5 & V6, usually a/w T inversion NSR No change NSSTTW Abnormal ECG Confounding Thrombolysis - +/- QS complexes in II, III & AVF from old ECG pattern ECG Rely on clinical hx for dx • Q waves • LBBB • ST changes • VPR - T waves in Rt to mid precordial and inferior leads have convex upwards shape • T wave • LVH mimicking hyperacute T waves of early MI changes Serial ECG & CE if indicated Dx Clinical Pathway in STE Rule of Appropriate Discordance ( in BBB or VPR) ST Leads with mainly negative QRS complexes (ie QS or rS complexes) 1) NSR – normal sinus rhythm segment should have STE 2) NSSTW (Non-specific ST segment/T wave abnormalities) Leads with mainly positive QRS complexes (ie large monophasic R waves) - ST elevation/depression of <1mm should have ST depression - Blunted/flattened/biphasic T waves w/o inversion or hyperacuity T wave T waves in leads with mainly negative QRS complexes have convex - Low risk of AMI upward or tall vaulting shapes similar to hyperacute T waves in early MI - but high risk of non-AMI ACS T waves in leads with mainly positive QRS complexes are frequently 3) Abnormal ECG inverted - ST changes, T inversion, Q waves Loss of this normal QRS complex-T wave axes discordance imply an acute 4) Confounding ECGs (LBBB, VPR, LVH) process eg AMI - ability to detect ACS is limited due to the abnormal repolarisation that accompany these patterns of abnormal intraventricular conductions d) LVH - Definition: voltage criteria V1 S wave + V5/6 R wave ≥35mm - Poor R wave progression
- 2. - V1 & V2: loss of septal R wave in Rt to mid precordial leads, usually resulting in QS pattern (ie mostly negative); usually a/w concave pattern STE and prominent T waves - Leads I, aVL, V5 & V6: ST depression with downsloping ST segment; prominent R waves; assymetrical (gradual downsloping initial limb with abrupt return to baseline), biphasic or inverted T waves Diagnostic Clinical Pathway in STE Overview 1) Identify chest pain patients with STE 2) For STE in LVH, BBB & VPR (ie confounding ECG patterns) - Use highly specific criterias to rule in AMI - If negative, use serial ECG to f/u the patient for dynamic changes suggestive of AMI 3) For STE in uncomplicated ECGs - Look for specific features to rule in AMI - If negative, use serial ECG to f/u the patient for dynamic changes suggestive of AMI Use of specific criterias aims to diagnose AMI quickly based on a single ECG so as to allow for rapid diagnosis and institution of thrombolysis/PCI. Digitally signed by DR WANA HLA SHWE DN: cn=DR WANA HLA SHWE, c=MY, o=UCSI University, School of Medicine, KT-Campus, Terengganu, ou=Internal Medicine Group, email=wunna. hlashwe@gmail.com Reason: This document is for UCSI University, School of Medicine students. Date: 2009.03.05 08:55:25 +08'00' Based on Clinical Decision-making in Adult Chest Pain Patients with Electrocardiographic ST-segment Elevation: STEMI vs Non-AMI Causes of ST- Segment Abnormality. William J Brady, Andrew Homer. Emergency Medicine
- 3. CP patient - Perform ECG STE ≥ 1mm in ≥2 contiguous leads a) VPR Sgarbossa Criteria – to rule in AMI in VPR Aim: Predict AMI in ECGs with confounding patterns (ie LVH, BBB, VPR) 1) Widened QRS (any one of 3) Yes STE ≥5mm with negative QRS complex? Likely MI – initiate Rx STE ≥1mm with positive QRS Positive ST depression ≥1mm with negative QRS Negative Serial ECG to look for dynamic changes No b) LBBB Sgarbossa Criteria – to rule in AMI in LBBB ≥0.2mm change in STE in single lead OR Positive Likely MI (any one of 3) ≥0.1mm change in STE in 2 leads Negative No ECG STE ≥1mm with positive QRS evidence of ST depression ≥1mm in V1,2 or 3 MI STE ≥5mm with negative QRS Sgarbossa Criteria is based on principle of appropriate discordance to look for abnormal ST segment changes It has low sensitivity & specificity, hence it is used to rule in PTs with MI in VPR/LBBB so as to allow for early initiation of Rx Does not rule out MI in VPR/LBBB, hence the need for serial ECG monitoring in PTs who do not meet Sgarbossa criteria. Aim is to look for dynamic changes that indicates ischaemic induced changes of an evolving AMI, as ST & T wave abnormalities are assumed to be temporally static in VPR/LBBB 2) Large amplitude LVH STE Concave up Serial ECG q4hr to look for dynamic changes 0.05mm change in STE or depression Yes QRS SV1 + RV 5/6 ≥ 35mm morphology Q wave devt High specificity Positive Likely MI T inversion in ≥2 anatomically continuous Negative No ECG but low sensitivity No leads evidence of - used to rule in Loss of ST segment concavity MI AMI, not to rule Convex up or Suspicious for MI out AMI obliquely flat ST segment morphology Convex upwards or obliquely flat 3) STE in Exclude AMI - specific but not sensitive, hence Yes used to rule in AMI Suspicious for AMI uncomplicated ECGs Aim: Predict AMI in uncomplicated ECGs Reciprocal ST depression Positive (in absence of LVH, BBB, - specific but not sensitive, hence VPR) used to rule in AMI Exclude Benign Early Repolarisation J point notching present Suspicious for AMI Exclude Acute Pericarditis PR depression OR Suspicious for AMI Ratio of ST height at J point in V6 to T wave apex height in V6 ≥0.25 Exclude AMI Ratio of sum off T wave apex heights in V1-4 Suspicious for AMI to sum of QRS apex heights in V1-4 >0.22 Serial ECG Positive Likely MI ≥0.05mm change in ST elevation or depression Negative No ECG Q wave devt evidence of MI T inversion in ≥2 anatomically continuous leads Loss of ST segment concavity