Overcoming Challenges in the Management of Moderate to Severe Atopic Dermatitis: Practical Strategies for Selecting Treatment for Pediatric and Adult Patients
•
0 recomendaciones•120 vistas

Chair Peter A. Lio, MD, prepared useful Practice Aids pertaining to atopic dermatitis for this CME activity titled “Overcoming Challenges in the Management of Moderate to Severe Atopic Dermatitis: Practical Strategies for Selecting Treatment for Pediatric and Adult Patients.” For the full presentation, downloadable Practice Aids, and complete CME information, and to apply for credit, please visit us at https://bit.ly/3uSsDSb. CME credit will be available until September 6, 2022.

Recomendados
Recomendados
Más contenido relacionado
Más de PVI, PeerView Institute for Medical Education
Más de PVI, PeerView Institute for Medical Education (20)
Último
Último (20)
Overcoming Challenges in the Management of Moderate to Severe Atopic Dermatitis: Practical Strategies for Selecting Treatment for Pediatric and Adult Patients
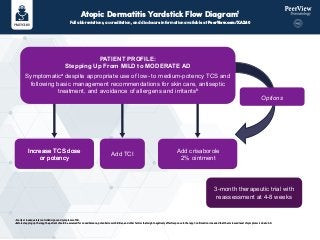
- 1. Atopic Dermatitis Yardstick Flow Diagram1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XAZ40 a Poorly or inadequately controlled signs and symptoms of AD. b Before stepping up therapy, the patient should be assessed for nonadherence, potential comorbidities, and other factors that might negatively affect response to therapy. Confirmation is needed that the increased level of symptoms is due to AD. PATIENT PROFILE: Stepping Up From MILD to MODERATE AD Symptomatica despite appropriate use of low- to medium-potency TCS and following basic management recommendations for skin care, antiseptic treatment, and avoidance of allergens and irritantsb Increase TCS dose or potency Increase TCS dose or potency Add TCI Add crisaborole 2% ointment 3-month therapeutic trial with reassessment at 4-8 weeks Options
- 2. Atopic Dermatitis Yardstick Flow Diagram1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XAZ40 Systemic immunosuppressant therapy Dupilumabd Phototherapyc 3-month therapeutic trial with reassessment at 4-8 weeks Cyclosporinee Methotrexatee Mycophenolate mofetile Azathioprinee Corticosteroidsf PATIENT PROFILE: Stepping Up From MODERATE to SEVERE AD Symptomatica despite an aggressive course of topical prescription therapy (TCS, TCI, crisaborole) for ≥3 wk; and following basic management recommendations for skin care, antiseptic treatment, and avoidance of allergens and irritants—particularly when there is a severe and negative impact on daily activities, psychosocial health, and QOLb Refer to specialist Consider for some patients acute tx to help gain control • Wet wrap therapy • Hospitalization a Poorly or inadequately controlled signs and symptoms of AD. b Before stepping up therapy, the patient should be assessed for nonadherence, potential comorbidities, and other factors that might negatively affect response to therapy. Confirmation is needed that the increased level of symptoms is due to AD. c The patient should be willing and able to commit to phototherapy in terms of cost, convenience, and access. d Indicated for patients aged ≥18 years with moderate to severe AD. It is the authors' expert opinion that dupilumab has a safety and efficacy profile that is better than that of immunosuppressive agents or phototherapy; cost and coverage are extremely important considerations. Documentation of the patient's disease severity, prior therapies, including failures, and impact on quality of life might be required. e Not FDA approved to treat AD. f FDA approved to treat AD but not recommended for long-term maintenance. A short course of systemic corticosteroids can help resolve severe symptoms, but exacerbation at discontinuation is common. Systemic corticosteroids also can be used as cotreatment during the initiation and optimization of phototherapy, other systemic immunosuppressants, and/or dupilumab. 1. Boguniewicz M et al. Ann Allergy Asthma Immunol. 2018;120:10-22.
- 3. Importance of Patient Education in Atopic Dermatitis Treatment Selection1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XAZ40 1. Simpson E et al. J Am Acad Dermatol. 2017;77:623-633. For patients with moderate to severe atopic dermatitis (defined by lesional severity and extent and/or significant impact on QOL, including social, emotional, and school/professional functioning) Systemic therapy Choice depends on childbearing capacity, comorbidities (ie, renal dysfunction, diabetes, alcohol abuse), age, and preferences (eg, injection vs tablets) Have you given intensive therapy an adequate trial? • Appropriate amounts of medium- to high-potency topical anti-inflammatory therapy for 1-4 wk followed by proactive therapy for maintenance • Consider wet wrap therapy and soak-and-seal Does the patient still have persistent, moderate to severe disease/impaired QOL despite intensive topical therapy? Consider phototherapy in selected patient groups Is phototherapy unsuccessful, unsuitable, and/or unavailable? Have you provided adequate patient education, including • Avoidance of irritants and known triggers? • Importance of adherence? • Optimized topical therapy (under- and overtreatment)? • Topical steroid phobia? • Structured educational intervention (eczema school)? Have you considered alternate diagnoses? • Have you managed infections? – Bacterial, viral, yeast • Have you considered patch testing for contact allergy? • Is referral to allergy services required for further testing and optimization of allergic rhinitis/asthma management?
- 4. Referring Patients With AD to Specialty Care1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XAZ40 1. https://atopicdermatitis.net/finding-healthcare-provider-doctor-specialist Dermatologists provide expertise in cases of AD that can be difficult to diagnose or treat. In certain patients, consultation with a pediatrician and/or allergist might also help. There are frequent flare-ups or there is severe AD Contact dermatitis is suspected There is a need for systemic therapies There is an uncertain diagnosis Attempts at managing the condition have not controlled the symptoms The patient has AD on the face that has not responded to treatment AD is causing significant psychosocial disturbances, including sleep disruption or reduced attendance at work or school For patients with chronic conditions such as AD, having a PCP instead of utilizing an urgent care facility for acute needs means the patient’s entire history and background will be taken into consideration.