8. – Sleep
– Satiety
– Stress&Exercise
– Sex
– Second half Menstrual cycle(luteal phase)
– Suckling
If a woman's prolactin level is elevated the first time it is tested,
a second sample should be checked when she is fasting and
non-stressed.
Physiologic conditions
13. •A craniopharyngioma is a benign tumor that
develops near the pituitary gland .
• most commonly in childhood and adolescence
and
•in later adult life.
compresses the pituitary stalk or gland, the tumor
can cause partial or complete pituitary hormone de
ficiency.
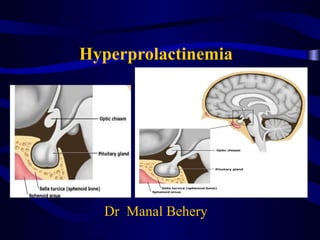
14. Diagrammatic representation of empty sella syndrome.
A, Normal anatomic relationship.
B, C, and D, Progression in development of empty sella syndrome.
Note thinning of floor and symmetric enlargement of sella turcica.
Empty sella sydrome
20. A- Inhibition of pulsatile GnRH secretion
1- Hyperprolactinemia inhibit GnRH activity by
interacting with hypothalamic DA and opioid
system via the short-loop feedback mechanism.
24. D- Inhibition of progesterone synthesis
4-Impaired ovarian strediogensis
25. Clinical Manifestation
• 1- Galactorrhea: Only in 30- 60 % of cases of
hyperprolactinemia due to :
• 2- Infertility: due to:- Anovulation luteal
phase defect
• 3- Oligohypomenorrhea , even amenorrhea
• 4- Hirsutism due to decreased SHBG.
• 5 -Decreased libido &osteoporosis
37. 3- Trans-sphenoid surgery:
• For Pituitary adenoma only if :
• - No response to medical ttt.
• - Causing visual field defect.
• - TTT is not tolerable.