
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Hydrocephalus
Similar a Hydrocephalus (20)
Último
Último (20)
Hydrocephalus
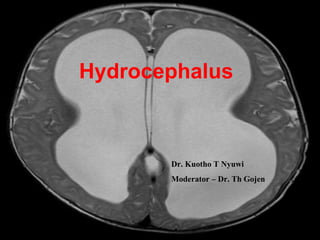
- 1. Hydrocephalus Dr. Kuotho T Nyuwi Moderator – Dr. Th Gojen
- 2. Definition: Abnormal collection of cerebrospinal fluid (CSF) resulting in abnormal widening of spaces in the brain Greek word: Hydro - Cephalus
- 3. Physiology and circulation of CSF - Normal volume of circulating CSF is around 150ml - Daily production is about 500ml/day, 20ml/hr Function: - Protects and support the brain and spinal cord. -Transport medium for transmitters and as a method of removing the end-products of metabolism.
- 6. Imbalance excessive accumulation of CSF Hydrocephalus - Excessive production - Decreased absorbtion - Obstruction
- 8. Etiology % Intraventricular hemorrhage 24 Myelomeningocele 21 Brain tumors 9 Aqueduct stenosis 7 CSF infection 5 Head injury 2 Others 11 Unknown 12
- 9. Types of hydrocephalus 1. Communicating and Non-communicating 2. Acute and chronic 3. Congenital and acquired Hydrocephalus Ex Vacuo Arrested hydrocephalus
- 10. Non-communicating (obstructive): CSF circulation is blocked at or proximal to fourth ventricular outlet foramina.(enlargement of ventricles proximal to the block) – Aqueduct stenosis, tumors Communicating (non-obstructive): At the level of the cisterns, the subarachnoid space or the level of the arachnoid granulation - Post meningitis, post hemorrhagic
- 11. 1. Congenital : Present at birth or few weeks/months after birth (1-2/1000 live births) Aqueduct stenosis Chiari malformations Dandy-Walker malformation 2. Acquired Infection (post-meningitis) Post – hemorrhagic (SAH,IVH) Tumors
- 12. 1. Acute : Develops within days or few weeks - Manifests with rapid progression of symptoms - Requires early attention and treatment hydrocephalus caused by tumor 2. Chronic : Over months (or even years) - Subtle signs of memory impairment, walking difficulty, urinary incontinence - A classic example is NPH Chronic hydrocephalus can present acutely because of changes in the pathophysiology of the CSF absorption or flow.
- 13. Structural characteristics - Dilatation of temporal and frontal horns of the lateral ventricles - Enlargement of ant. or post recesses of 3rd ventricle - Narrowing of ventricular angle - Effacement of cortical sulci
- 14. Clinical Features Due to increased ICP and dilation of ventricles, causing compression of the adjacent brain In neonatal period Skull - thin and relatively non rigid allows for an overall cranial expansion Craniofacial disproportion Irritable Fussy May not accept feeds Vomiting Poor head control Lethargy Drowsiness In extreme cases, lapse into a comatose state
- 15. Cont…. - Fontanel full , bulging and wide - Thin and glistening scalp with enlargement and engorgement of scalp veins - Macewen's sign ( cracked pot sound on head percussion) - Sixth nerve (abducens) palsy - Setting sun sign - upward gaze palsy - Hyperactive reflexes. - Irregular respiration with apneic spells. - Separation of cranial sutures (sutures diastasis)
- 18. In older children and adults The enlarging ventricles result in raised ICP and compression of the adjacent brain 2 common modes of presentation a) rapidly progressive hydrocephalus b) chronic hydrocephalus.
- 19. Rapidly progressive hydrocephalus Increased ICP - new-onset headache and vomiting If untreated, these symptoms worsen and blurring of vision often occurs. In patients with long-standing raised pressure, papilledema can result If still untreated, drowsiness and progression to coma follow.
- 20. Chronic hydrocephalus - CSF accumulates more slowly - gradually compressing the brain - Predominantly seen in older adults - The patient becomes progressively dull, apathetic, and uninvolved with the surroundings. - Memory impairment for recent events is commonly seen, but usually the remote memory is well preserved.
- 21. - Short stepped gait with a wide stance and unsteadiness - Urinary incontinence - No significant headache Cerebellar fits or hydrocephalic attacks: (severe headache, patient lapses into sudden unconsciousness associated with a decerebrate or decorticate response, downward deviation of the eyeballs, and respiratory distress) Medical emergency
- 22. Investigation Ultrasonography to visualize the ventricular system(when the anterior fontanelle is patent) CT /MRI of the head LP in cases of communicating hydrocephalus for both diagnostic and therapeutic
- 23. Management The ultimate goal is to reverse the neurologic damage caused by the raised ICP Medical treatment - not proved to be useful Used as a temporary measure and in conjunction with surgical management. Acetazolamide - Commonly used - reduce CSF production. However, benefits are minimal and high doses of the drug, which cause metabolic acidosis, are required to achieve the effect.
- 24. Surgical Involves diversion of the accumulated CSF (1) by reopening the obstruction to allow the CSF to flow into its natural pathway (2) by creating a diversion before the obstruction to allow the CSF to drain into the intracranial pathways distal to the block (3) by diversion of the CSF into another cavity so it becomes absorbed into the bloodstream. Removal of obstruction like posterior fossa tumor
- 25. Although shunts have been the mainstay of treatment for several decades, endoscopic procedures have now become more popular. These include: i) Endoscopic third ventriculostomy- into the basal cisterns ii) Endoscopic aqueductoplasty – 3 fr forgarty catheter iii) Endoscopic aqueductal stenting.
- 26. CSF diversion procedure : - Children <5 years : difficult to assess intellectual development - Protects against the effects of persistent ventriculomegaly and ensures an optimal environment for future intellectual development - >5 years and adults with asymptomatic ventriculomegaly often are closely watched, with frequent assessment of intellectual development, before considering a shunt insertion.
- 27. Cerebrospinal Fluid Shunts -Ventriculo-peritoneal(VP) - most common -Ventriculo-atrial(VA) -Torkildsen shunt (in aqueduct stenosis by passing a catheter from the lateral ventricles into the cisternal space) -Lumbo-peritonial shunt. -External drainage – temporary
- 29. Complications of shunts Shunt malfunction Infection Obstruction. Acute hemorrhages Over drainage Hematoma Disconnections Seizure Distal Complication Ascitis Pseudoperitoneal cyst
- 30. Normal-Pressure Hydrocephalus - Older patients with excessive accumulation of the CSF in the intracranial compartment leading to dilation of the ventricles and subarachnoid spaces - The clinical picture is typically of an older patient who presents with the triad of gait ataxia, dementia, and urinary incontinence
- 31. Exact cause unknown - reduced absorption -ICP not usually raised - brain parenchyma is less stiff to allow it to be compressed by the developing ventriculomegaly -Diagnosis: combination of clinical features with prominent ventricles seen by CT /MRI, with no other abnormalities. - A therapeutic trial of CSF drainage has been used for patients suspected of having NPH to predict response to treatment.
- 32. Treatment Diversion of CSF: i) ventriculoperitoneal shunt ii) lumboperitoneal shunt
- 33. Thank you