
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Coloboma
Similar to Coloboma (20)
More from Dr. Shah Noor Hassan
More from Dr. Shah Noor Hassan (20)
Recently uploaded
Recently uploaded (20)
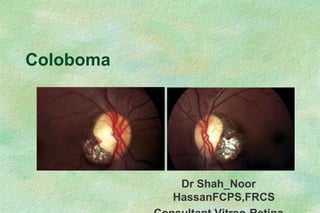
Coloboma
- 2. Definition Koloboma (in Greek) – Mutilated or curtailed. Primarily its a embryologic defect. Malformation refers to a notch, gap, hole, or fissure in any of the ocular structures.
- 3. Demography Most cases are sporadic Incidence – 0.14% Usually bilateral - 60% Complicated by RRD. RRD – 40% in lifetime. Congenital, developmental ocular defect – associated with iris coloboma, microphthalmous, high myopia, glaucoma, cataract and phthisis bulbi.
- 4. 3 embryonic layers: The neural ectoderm - optic vesicle and optic cup. Surface ectoderm Cranial neural crest minor contribution from the mesoderm (striated extraocular muscles and vascular endothelia). EMBRYOGENESIS (RPE, the iris sphincter and dilator muscles, the posterior iris neuro-epithelium, the pigmented and nonpigmented ciliary epithelium, and the optic nerve fibers and glia) The lens, the corneal epithelium, the lacrimal gland, the surface epidermis of the lids and the epithelium of the adnexal glands and conjunctiva . Corneal keratocytes, endothelium and trabecular meshwork; the iris and choroidal stroma, including pigmented and nonpigmented cells; the ciliary smooth muscle; the fibroblasts of the sclera; and the optic nerve meninge
- 5. GENESIS of COLOBOMA • 5th to 7th week of fetal life (7–14 mm stage) • Closure – Inferior midline from equator Faulty closure results in a area with absence of uveal tissue and RPE. … Coloboma
- 7. HISTOLOGY Total absence of the RPE and Choroid. (Rarely /Occasionally choroidal vessel may be seen to traverse the colobomatous defect). The sensory retina is very thin (Rudimentary retinal tissue - abnormal, underdeveloped, undifferentiated, diaphanous, flimsy,anomalous and maldeveloped).
- 9. TYPES 1. TYPICAL / ATYPICAL 2. COMPLETE / INCOMPLETE 3. LENS COLOBOMA 4. POSTERIOR SEGMENT COLOBOMA
- 10. 1. TYPICAL 2. ATYPICAL TYPICAL Inferonasal – most frequent. May affect any part of the globe –traversed by the fissure from iris to the optic nerve.
- 11. Located anywhere other than in inferonasal quadrant ATYPICAL
- 12. 2. COMPLETE / INCOMPLETE Full thickness defect, involving both the pigment epithelium and the iris stroma. Total - Extending to the iris root and giving rise to the “keyhole pupil. Partial – Involving only the pupillary margin and causing a slightly oval pupil. COMPLETE:
- 13. Partial thickness, involving either the pigment epithelium or the iris stroma. Wedge shaped and best demonstrated by iris transillumination. Heterochromia iridis and colobomata have occurred simultaneously. INCOMPLETE:
- 14. 3. LENS COLOBOMA - a coloboma of the zonule and/or ciliary body a misnomer because there is no actual loss of lens substance. Segmentally defective or absent development of the zonules.
- 15. 4. POSTERIOR SEGMENT COLOBOMA A. Choroidal coloboma B. Optic disc coloboma C. Macular coloboma
- 16. A. Choroidal coloboma Types: Ida mann classification
- 17. Types: Ida mann classification 4 5 1 2 3 6 7
- 18. Atypical and unrelated to choroidal fissure closure. Bilateral, symmetrical, circumscribed and excavated defects that involve both the choroid and retina. B. Macular colobomata
- 19. Classified : 1. Pigmented 2. Nonpigmented 3. Associated with abnormal vessels B. Macular colobomata
- 21. C. Optic disc coloboma • Rare, unilateral or bilateral • Usually sporadic - occasionally dominant • VA – decreased (Depends on severity). • Large disc with inferior excavation • Superior visual field defects • Associated with other colobomas •
- 22. • Optic disc involvement has been classified into six types, increasing in severity from a normal disc outside the chorioretinal coloboma as the mildest form to a nonidentifiable disc shape with blood vessels emerging from the superior border of a large chorioretinal coloboma. •This classification is helpful forThis classification is helpful for predicting the degree of visual impairment in optic disc colobomata, particularly in infants and young children whose visual acuity can be difficult to measure.
- 24. Asymptomatic Leucocoria - early in life Loss of central vision (useful peripheral vision may be preserved if the lesion is small). Visual field defect - not noticed by the patient Visual loss - RD
- 25. Vision depends - Involvement of the optic nerve, macula, and papulomacular bundle. Bilateral cases - poor visual function and nystagmus. Unilateral cases - a sensory strabismus, with superimposed “organic amblyopia. Asymptomatic - macula is spared and the optic nerve and papulomacular bundle are not severely involved
- 26. SIGNS Inferonasal "key hole" pupil may be seen if iris is involved Amblyopia Visual field defects Relative afferent pupillary defect (RAPD) Associated microphthalmia
- 27. Choroidal coloboma Fundus coloboma Glistening white with definable borders, frequently with irregular clumps of pigment along the rim.
- 28. Margins - Variations Choroidal coloboma
- 29. Area of bare sclera devoid of overlying normally differentiated retina or choroid. Undifferentiated retinal remnants may persist as a membrane, sometimes with associated retinal vessels. Choroidal coloboma
- 30. Enlarged, white, sharply delineated, bowl-shaped excavations 2–8 diopters in depth Rim of neural tissue - preserved superiorly Six types – Severity of disc involvement Optic disc coloboma
- 31. Macular colobomata Bilateral, symmetrical, circumscribed and excavated defects that involve both the choroid and retina.
- 32. COMPLICATIONS
- 33. COMPLICATIONS Retinal detachment - most common Cataract and Lens subluxation Subretinal neovascularization causing serous macular detachment Secondary glaucoma Amblyopia, Nystagmus Anisometropia, and Sensory strabismus
- 34. RD in Coloboma RRD – 40% in lifetime 0.6–1.7% are associated with retinochoroidal coloboma. Congenital RD – incomplete attachment Acquired RD– more common RRD/ Non-RRD
- 35. PATHOGENESIS OF DETACHMENT Rudimentary retinaAbnormal preretinal tissue Tractional process break formation. Extremely thin minimal changes Atrophic hole retinal pigment epithelial pump - missing Myopic Vitreous Syneresis
- 36. Histologic sections – RRD in Coloboma Inner layer break - Central Retinal vascular ischemia or scleral stretching could explain the break in the inner layer. Outer layer break - at the margin of the coloboma Secondary either to vitreous traction at the margin or Extension of an initially isolated detachment to the margin of the coloboma, where there is less glial support.
- 37. Subtle defects in the lens/zonule/ciliary body complex. Fluid can gain access to the subretinal space through a break in the nonpigmented epithelium of the ciliary body. PATHOGENESIS OF DETACHMENT – contd…
- 38. Non- RRD and Retinoschisis associated with Choroidal & disc coloboma Dome-shaped macular detachment * with an outer lamellar macular hole with irregular margins # surrounded by a schisis-like separation between the inner and outer retina †. Note the optic and adjacent choroidal coloboma.
- 39. Outer lamellar macular hole may be secondary to chronic cystoid macular oedema KAZUKI HOTTA etal Br J Ophthalmol 1999;83:123 ( January ) PATHOGENESIS
- 40. Finding of breaks – Difficult d/t (1) The rudimentary retina is extremely thin, (2) The breaks are usually atrophic holes without the presence of flaps or operculae (3) The white background of the sclera (4) The tiny breaks may be hidden under the overhanging edge of the coloboma, and (5) Tiny breaks may be hidden in areas of hemorrhage.
- 41. Cataracts Pigment clumping on the lens capsule at the equator. Subcapsular and cortical opacification, anterior and posterior polar cataracts, and total opacification. Lens subluxation USG
- 42. USG
- 43. SRNVM causing serous macular detachment Develops - Superotemporal edge of the coloboma Comparable to the CNVM associated with high myopia, angioid streaks, choroidal ruptures.
- 44. Predisposition: Abrupt termination and abnormal architecture of the RPE and Bruch’s membrane at the margin. Treatment with laser photocoagulation. SRNVM causing serous macular detachment
- 45. MANAGEMENT
- 46. Evaluation Lack of cooperation, nystagmus and micropthalmos - EUA in children's SLE & Fundus Evaluation Accurate refraction & BCVA Ultrasonography Fields
- 47. TREATMENT Treatment of refractive error and amblyopia, if present Low vision (vision rehabilitation) services, if indicated Associated - Cataract,RD orCNV :treated accordingly
- 48. Iris defects Impose no visual defect cosmetic contact lens Surgical treatment as part of cataract extraction / penetrating keratoplasty Repaired with nonabsorbable sutures. Iris prosthesis
- 49. Iris defects Zonular integrity is insufficient Haptics should be placed 90 degrees from the defect Cataract and microphthalmia may be complicated by postoperative : uveal effusion, retinal detachment, intraocular hemorrhage, and malignant glaucoma
- 50. RETINOCHOROIDAL COLOBOMA Prophylactic Laser treatment – posteriorly along the edge of the coloboma and Cryopexy anteriorly
- 51. TREATMENT of RRD RD Outside coloboma - Conventional scleral buckling techniques. - Vitrectomy + intraocular tamponade in complicated cases. RD Involving Coloboma - Buckling (Low Success rate) - Vitrectomy + EL + SOI
- 52. External buckling has a low success rate (35 -57%) - Difficulty in identifying breaks, - Posterior location of the breaks, - Impossible to flattened the anomalous retina - Inability to create a surrounding retinopexy (cryotherapy or laser photocoagulation). TREATMENT of RRD contd…
- 53. Wang et al . Tr. Am. Ophth Soc. vol. LXXXIII, 1985 Better Results::: Radial Buckles: - One/Two buckle/s - Length depends on length of coloboma Retinopexy surrounding coloboma
- 54. Preferred modality -Vitreous surgery Vitrectomy + Intraocular Gas Vitrectomy + SOI Vitrectomy + PFCL Encirclage + Vitrectomy + Intraocular tamponade
- 55. SURGICAL TECHNIQUE PARS PLANA VITRECTOMY PARS PLANA LENSECTOMY-where ever required. Induction of PVD and MP ( membrane peeling) wherever required. Use of wide angle visualisation system and magnification of microscope
- 56. Vitrectomy With Cyanoacrylate Retinopexy Cyanoacrylate retinopexy at regions suspected of retinal break. Endophotocoagulation around the disc or at the papillomacular bundle was avoided. Kazuki Hotta etal . The Management of Retinal Detachments Associated With Choroidal Colobomas by Vitrectomy With Cyanoacrylate Retinopexy Japanese J Ophthalmol Vol 42,Issue 4, July 1998, Pages 323-326 (E search)
- 58. DIFFERENTIAL DIAGNOSES Morning glory disk anomaly Chorioretinal scar Staphyloma (idiopathic, myopic, or associated with connective tissue disorder). North Carolina macular dystrophy
- 59. Morning glory disk anomaly Paracentral defect, typically inferior Annular zone of pigmentary disturbance Anomalous retinal vessels and a central glial tuft.
- 60. OPTIC NERVE PITS Crater-like holes or indentations in the surface of the optic disk Frequently seen- temporal aspect of the disk incidence is approximately 1:10,000 incomplete or partial colobomata – Atypical 57% in the left eye and 43% in the right
- 61. Histologically Herniations of dysplastic retina into a collagen-lined pocket, which often extends posteriorly into the subarachnoid space through a defect in the lamina cribrosa. Edema and cystoid degeneration of the outer plexiform layer - macula OPTIC NERVE PITS
- 62. Etiology - faulty closure of an aberrant fetal fissure Asymptomatic Associated with CSR or Serous retinal detachment or R’Schisis Communication between the vitreous and/or retina and the subretinal space may develop. OPTIC NERVE PITS
- 63. Differential diagnosis: healed toxoplasma choroiditis healed chorioretinitis secondary to Toxocara canis Macular colobomata
- 65. Scarred SRNVM
- 66. Bilateral colobomas Symmetric location
- 67. Chorioretinitis scar Asymmetric location
- 68. Iris coloboma
- 69. Systemic Associations of Coloboma 1. CNS malformation - basal encephalocele and cysts 2. Chromosomal anomalies - Patau syndrome (trisomy 13) and cat-eye syndrome (trisomy 22) 3. ‘CHARGE’ - Coloboma, Heart defects, choanal Atresia, Retarded development, Genital and Ear anomalies 4. Other syndromes - Meckel-Gruber, Goltz, Lenz microphthalmos, Walker-Warburg and Goldenhar
- 70. Conclusion Often associated with microphthalmia. Isolated ocular anomaly or in association with multisystem anomalies Wide variation in severity Treatment is dependent on location and severity A genetic evaluation is warranted in all cases
- 71. RF data Jan 2006 to 2010 Fourty six eyes of 45 patients with retinal detachments related to coloboma of the choroid were analyzed. All eyes underwent through various procedure for retinal detachment surgery..
- 72. Patient characteristic N46 NO % AGE MEAN 21.9Year RANGE 7-40 Year SEX MALE 31 67.4 FEMALE 15 32.6 COLOBOMATOUS EYE RE 6 13 LE 6 13 BOTH 34 74 COLOBOMATOUS EYE WITH RD RE 22 47.8 LE 18 39.2 BE 6 13
- 73. SURGICAL PROCEDURES NO. OF PATIENTS % ENCIRCLAGE+BMV+SOI 18 39.1 CATRACT/LENSECTOMY+ENCIRCLAGE +BMV+SOI 10 21.7 BMV+SOI 9 19.6 BMV+C3F8 1 2.2 RD SURGERY 8 17.4
- 74. SURGICAL PROCEDURES NO. OF PATIENTS % SOR RE RD % OF Re RD %Of Re RD After SOR 1. ENCIRCLAGE+BMV+SOI 18 39.1 8 3 16 37.5 2. CATRACT/LENSECTOMY + ENCIRCLAGE +BMV+SOI 10 21.7 4 2 20 50 3. BMV+SOI 9 19.6 4 1 11 25 4. BMV+C3F8 1 2.2 _ 1 100 -- 5. RD SURGERY 8 17.4 _ 3 37.5 --
- 75. BEST CORRECTED VISUAL ACUITY AT LAST FOLLOW UP BEST CORRECTED VISUAL ACUITY NO.OF PATIENTS % 20/20 –20/40 1 2.1 20/60—20/120 6 13.0 20/200—10/200 27 58.9 3/200—COUNTING FINGER 5 10.9 HEND MOVEMENT—PERCEPTION OF LIGHT 6 13.0 NO PERCEPTION OF LIGHT 1 2.1 46 100
- 76. Thanks