Psoriasis management of ayurveda
•Descargar como PPTX, PDF•
23 recomendaciones•4,945 vistas

Psoriasis management of ayurveda

Recomendados
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (14)
Similar a Psoriasis management of ayurveda
Similar a Psoriasis management of ayurveda (20)
Más de Dr. Ruchi Gulati,MD(Ayurveda)
Último
Último (20)
Psoriasis management of ayurveda
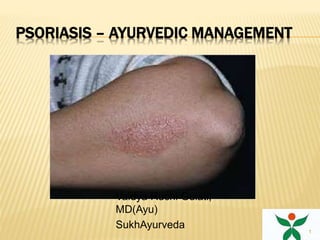
- 1. PSORIASIS – AYURVEDIC MANAGEMENT Vaidya Ruchi Gulati, MD(Ayu) SukhAyurveda 1
- 2. OVERVIEW 5. Summary 2 4. Managing psoriasis 3. Diagnosing psoriasis 2. Clinical presentation 1. Introduction
- 3. WHAT IS PSORIASIS? Inflammatory and hyperplastic disease of skin Characterised by erythema and elevated scaly plaques Chronic, relapsing condition Course of disease often unpredictable 3
- 4. PSORIASIS 4
- 5. EPIDEMIOLOGY Common skin disorder Prevalence variable: ~ 0.3–2.5% Prevalence equal in males and females Estimated incidence: ~ 60 per 100,000 per year 5
- 6. AGE OF ONSET Mean age: ~ 23–37 years Current theory: 2 distinct peaks with possible genetic associations Early onset (16–22 years) More severe and extensive More likely to have affected first-degree family member Late onset (57–60 years) Milder form Affected first-degree family members nearly absent 6
- 7. PSORIASIS IS A T-CELL MEDIATED, AUTOIMMUNE DISEASE1 Current hypothesis: Unknown skin antigens stimulate immune response Antigen-specific memory T-cells are primary mediators Leads to impaired differentiation and hyperproliferation of keratinocytes 7
- 8. COMMON TRIGGER FACTORS FOR PSORIASIS Infections (e.g. streptococcal, viral) Skin trauma (Koebner phenomenon) Psychological stress Drugs (e.g. lithium, beta blockers) Sunburn Metabolic factors (e.g. calcium deficiency) Hormonal factors (e.g. pregnancy) 8
- 10. CLINICAL PRESENTATION: CLASSIC PSORIASIS Well-defined and sharply demarcated Round/oval- shaped lesions Usually symmetrical Erythematous, raised plaques Covered by white, silvery scales 10
- 11. COMMON SITES AFFECTED BY PSORIASIS Can affect any part of the body – typically scalp, elbow, knees and sacrum Extent of disease varies 1 11
- 13. TYPES OF PSORIASIS Chronic plaque Guttate Flexural Erythrodermic Pustular Localised and generalised Local forms Palmoplantar Scalp Nail (psoriatic onychodystrophy) 13
- 14. CHRONIC PLAQUE PSORIASIS Most common type – affects approximately 85% Features pink, well- defined plaques with silvery scale Lesions may be single or numerous Plaques may involve large areas of skin Classically affects elbows, knees, buttocks and scalp 14
- 19. GUTTATE PSORIASIS Numerous and small lesions – ~ 1 cm diameter Pink with less scale than plaque psoriasis Commonly found on trunk and proximal limbs Typically seen in individuals < 30 years Often preceded by an upper respiratory tract streptococcal infection 1. 19
- 20. FLEXURAL PSORIASIS Lesions in skin folds articularly groin, gluteal cleft, axillae and submammary regions Often minimal or absent scaling May cause diagnostic difficulty when genital or perianal region is affected in isolation 1 20
- 21. ERYTHRODERMIC PSORIASIS Generalised erythema covering entire skin surface May evolve slowly from chronic plaque psoriasis or appear as eruptive phenomenon Patients may become febrile, hypo/hyperthermic and dehydrated Complications include cardiac failure, infections, malabsorption and anaemia Relatively uncommon 21
- 22. PUSTULAR PSORIASIS Two forms: Localised form More common Presents as deep-seated lesions with multiple small pustules on palms and soles Generalised form Uncommo Associated with fever and widespread pustules across the body inflamed body surface 22
- 23. PALMOPLANTAR PSORIASIS Can be hyperkeratotic or pustular May mimic dermatitis – look for psoriatic manifestations elsewhere to aid diagnosis Possibly aggravated by trauma 23
- 24. SCALP PSORIASIS Varies from minor scaling with erythema to thick hyperkeratotic plaques May extend beyond hairline Patient scratching may produce asymmetric plaques 24
- 25. NAIL PSORIASIS May be present in patients with any type of psoriasis Can take several forms: Pitting: discrete, well- circumscribed depressions on nail surface Subungual hyperkeratosis: silvery white crusting under free edge of nail with some thickening of nail plate Onycholysis: nail separates from nail bed at free edge ‘Oil-drop sign’: pink/red colour change on nail surface 25
- 27. PSORIATIC ARTHRITIS Approximately 5–20% have associated arthritis Five major patterns of psoriatic arthritis: Distal interphalangeal involvement Symmetrical polyarthritis Psoriatic spondylarthropathy Arthritis mutilans Oligoarticular, asymmetrical arthritis Clinical expressions often overlap 27
- 28. DIAGNOSING PSORIASIS Other dermatological disorders can resemble psoriasis Diagnosed clinically according to appearance, distribution, history of lesions and family history Important to consider non-cutaneous complications 28
- 29. DIFFERENTIAL DIAGNOSIS Localised patches/plaques Tinea Eczema Superficial basal cell carcinoma and Bowen’s disease Seborrhoeic dermatitis Cutaneous T-cell lymphoma (mycosis fungoides) Guttate Pityriasis rosea Drug eruption Secondary syphilis Flexural Tinea Eczema Candidiasis Seborrhoeic dermatitis Erythrodermic Eczema Cutaneous T-cell lymphoma Pityriasis rubra pilaris Lichen planus Drug Palmoplantar Tinea 29
- 30. CLINICAL APPROACH Dosha chikitsa -Vatakapha/kapha/vata/pitta Dushya chikitsa -Rasa, Rakta Prasadana Avasthanusara Chikitsa -Saama/Niraama -Navina/ Jirna Vyadhi pratyaneeka chikitsa Manobala vardhaka chikitsa Rasayana(Naimittika) 30
- 31. MANAGING PSORIASIS Goals of management Tailor management to individual and address both medical and psychological aspects Improve quality of life Achieve long-term remission and disease control Minimise drug toxicity Evaluate and monitor efficacy and suitability of individual treatments Remain flexible and respond to changing needs 31
- 32. MANAGING PSORIASIS Before starting treatment Establish relationship of trust with patient Provide patient with information Emphasise benign nature of disease Explain that psoriasis tends to be chronic and recurrent 32
- 33. TREATING PSORIASIS: GENERAL MEASURES Reduce/eliminate potential trigger factors: Stress Smoking Alcohol Trauma Drugs Infections 1 33
- 34. FACTORS FOR SELECTION OF TREATMENT Age: childhood, adolescence, young adult hood, middle age,>60 yrs Type of psoriasis: Plague, palmar, generalised pustular, etc Site and extent of involvement: localised to scalp, palms, scattered plaques but <5% involvement: generalised and >30% involement. Previous treatment: Systemic glucocorticoids, methotrexate Associated medical disorders(eg. HIV, CVD) Duration of Disease: <1month, <1 yr, >1yr 34
- 35. PROTOCOL-1 Mild symptoms Recent origin Localized 35
- 36. CHIKITSA Sadya Virechana with Avipatti choornam-20gms for 1day if saama lakshanas are seen - Shaddharana(5gm) / panchakola choorna) Mahatiktakam kashaya - 15ml bd for 1st week Kaisoraguggulu - 1 tab bd for first week Manasamitra vataka - 1 tab bd for 2 weeks Gandhaka rasayan - 100mg with honey bd (throughout) Vitpala kera taila - external application followed by sun exposure 36
- 37. PROTOCOL 2 MODERATE SYMPTOMS HISTORY OF 2-6 MONTHS AFFLICTED TO A LARGER AREA 37
- 38. CHIKITSA Mahatiktakam ghrutha -15 gm(inc acc to agni bala X 7 days for snehan (along with Abhyangam and sarvanga swedanam) SadyoVirechana with Avipatti choorna - 20gm for 1st week. Tiktakam kashaya - 15ml bd X 2 weeks ( if saama lakshanas are seen - 5-6gm shaddharana choorna /gutika) Kaishore Guggulu - 1 tab tds X 2 weeks Arogya vardhini gutika - 1 tab tds X 2weeks Gandhaka Rasayan- 100mg with honey (throughout) Haridrakhandam -12gm bd X 2weeks Manasmitra vatakam – 2 tabs bd X 2weeks Vitpala kera taila - external application followed by sun exposure 38
- 39. EXTERNAL TREATMENTS Vitpala kera taila Vitpala snana/Sidharthaka snana choorna Takra dhaara (musta,amalaki) 39
- 40. PROTOCOL 3 SEVERE SYMPTOMS HISTORY OF 6 MONTHS AND MORE SPREAD EXTENSIVE AREAS WITH SEVERE MENTAL STRESS 40
- 41. CHIKITSA Starting with the previous protocol according to the bala, avastha of Roga and Rogi, moving on to the additional treatments. Rookshana – Takra dhaara(musta,triphala,aragwadhadi) Deepana-pachana -Panchakola churna with takra/usna jala Snehapana -dose acc. to agni bala. (Mahatiktakam ghrutha/guggulutiktakam ghruta) Abhyangam - vitpala Swedana - usna jala snana, atapa sevan Nasya - shadbindu taila Vamana - madana,vacha,yashti,pippali+madhu Virechana - avipatti choorna/ trivrut leha 41
- 42. FOLLOW UP Need of Rasa-Rakta prasadana - Manobala vardhaka -Rasayana chikitsa. Rasa-Rakta parasadana Mahamanjishtadi kashaya. 15ml bd X 1 month Krumimudgar ras 1 hs X 1week Manasamitra vataka 1bd X 1 month Kalayana ghrutha 12gm hs X 1month Gandhaka Rasayana 1tab bd X 1month 42
- 43. PATHYA For a minimum of 3 months to control symptoms and relapse Ahara :Avoid Virudha, vidaahi , guru , abhishyandi, navaanna, matsya, anupa mamsa, kanda varga. : reduce the use of lavana : include more haridra, rasona, pepper in the diet. : avoid pickles, dadhi at night ,fermented food items. : avoid bakery items (maida), oily and spicy foods. : strictly avoid egg,beef and pork. : Avoid ready to cook items, tinned foods etc. : avoid re-cooking refrigerated foods. Vihaara : maintain hygiene in all aspects. : practice Achara rasayana. 43
- 44. MANAGEMENT OF PSORIASIS: SUMMARY Chronic, inflammatory disease of skin Classic presentation characterised by red, scaly plaques Management should address both medical and psychological aspects Treatments include externaltherapy, panchkarma, Rasa-Rakta prasadana - Manobala vardhaka -Rasayana chikitsa. Rasa-Rakta parasadana 44
- 45. THANK YOU ALL 45