Biomechanich of the spine ppt (2)
•
148 recomendaciones•60,965 vistas

SPINE BIOMECHANICS

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Biomechanich of the spine ppt (2)
Similar a Biomechanich of the spine ppt (2) (20)
Más de Dr.Debanjan Mondal(PT)
Último
Último (20)
Biomechanich of the spine ppt (2)
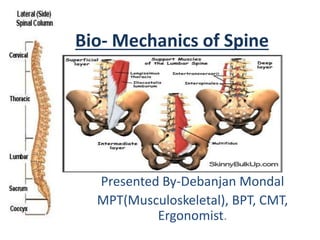
- 1. Bio- Mechanics of Spine Presented By-Debanjan Mondal MPT(Musculoskeletal), BPT, CMT, Ergonomist.
- 2. Introduction. • Spine or Vertebral Column or Backbone is a complex structure meant for support and a linking structure between upper and lower extremities. • It provides a base of support for the head and internal organs, a stable base for the attachment of ligaments, bones and muscles of the extremities, rib cage and the pelvis. • It is a link between the upper and the lower extremities and provide mobility for the trunk. • It protects the Spinal cord.
- 4. Structure; • The Spine comprises 33 vertebral bones and 23 Intervertebral disks. • Cervical (7), Thoracic (12), Lumbar (5), Sacral (5), Coccygeal (4) • The vertebrae increase in size from the cervical to lumbar region and decrease in size from the sacral to coccygeal region. • Vertebral column when viewed from the posterior aspect, all regions together present a single vertical line that bisects the trunk. • When viewed from the side, a number of curves are seen that vary with age . • Primary curve (Kyphotic curve)- Thoracic and Sacral, they retain the original posterior convexity throughout life. • Secondary curve (Lordotic curve)- Cervical and Lumbar, they develop as anterior convexity as a result of the accommodation of the skeleton to the upright posture.
- 5. Articulations • Two main types of articulations are found in the vertebral column: • (1)Cartilaginous joints of the symphysis type between the vertebral bodies and the interposed disks and • (2)Diarthrodial or Synovial joints between the zygopophyseal facets located on the superior articular processes of one vertebra and the zygopophyseal facets on the inferior articular processes of an adjacent vertebra above. • The joints between the vertebral bodies and disks are referred to as the Intervertebral joints. • The joints between the zygapophyseal facets are called the Zygapophyseal (apophyseal or facet) joints. • All the zygapophyseal joints, except for the joint between the first two cervical vertebrae, are plane synovial joints. • The vertebral column articulates with the ribs, with the skull and the pelvis at the sacroiliac joints.
- 6. • The motion between any two vertebrae at the intervertebral joints is extremely limited and consists of a small amount of gliding (translation) and rotation. • According to White and Punjabi, one vertebra can move in relation to an adjacent vertebra in six different directions ( 3 translations and 3 rotations) along and around three axes. • The compound effects of these small amounts of translation and rotation at a series of vertebrae produce a large range of motion for the column as a whole. • So Vertebrae has got 3 degree of freedom, permitting flexion and extension, lateral flexion and rotation. • However, motions in the vertebral column often are coupled motions. Coupling- the consistent association of one motion about an axis with another motion around a different axis. Eg. Axial rotation is coupled with lateral flexion and forward flexion)
- 7. A Typical Vertebra. • The structure of a typical vertebra consists of two major parts: an anterior cylindrically shaped vertebral body and a posterior irregularly shaped vertebral arch. • Vertebral body- is composed of a block of trabecular or spongy bone, which is covered by a layer of cortical bone. According to Wu and Chen, the stresses induced in the cortical bone shell are always much higher than in the trabecular bone and stresses induced in the vertebral body are always larger at the anterior side than on the posterior side. • The cortical covering of the superior and inferior surfaces or plateaus is thickened around the rim where the epiphyseal plates are located and in the center by a layer of hyaline cartilage called the cartilaginous end-plate. • The vertical, oblique and horizontal trabecular systems correspond to the stresses placed on the bodies. Vertical system sustain the body weight and resist compression forces while other trabecular systems help to resist shearing forces. • Areas of strength are the area where the trabeculae cross each other and the area of weakness is evident in the anterior portion of the body, which is a potential site for collapse of the vertebrae resulting compression fracture.
- 9. • The vertebral arch is a more complex structure than the body, because it has many projections, including 3 nonarticular processes and 4 articular processes. • Nonarticular processes are 2 transverse and 1 spinous process. They provide sites for the attachment of ligaments and muscles. The 2 transverse processes divide the arches into anterior and posterior portions. • The portions of the arch located anterior to the transverse processes are called Pedicles which attach the arches to the right and left upper posterior walls of the vertebral body. • The portions of the arches posterior to the transverse processes constitute the laminae. The posterior portions of the laminae that are located between the superior and inferior articular processes on each side are called the pars interarticularis where vertically oriented lamina and horizontally oriented pedicle meet.
- 10. Summary; Vertebral Function. Structure Function Body Resists compressive forces. Transmits compressive forces to vertebral end plates. Pedicles Transmit bending forces (exerted by muscles attached to the spinous and transverse processes) to the vertebral bodies Laminae Resist and transmit forces (that are transmitted from spinous and zygapophyseal articular processes) to pedicles. Serve as attachment sites for muscles and ligaments. Transverse processes Serve as attachment sites for muscles and ligaments. Spinous processes Resist compression and transmit forces to laminae. Serve as attachment sites for ligaments and muscles. Zygapophyseal facets Resist shear, compression, tensile and torsional forces. Transmit forces to laminae.
- 11. Intervertebral Disk • The intervertebral disks make up about 20% to 33% of the length of the Spine. ( approx. 70 cm in male, 60 cm in female) • The size increases from the cervical to the lumbar region and disk thickness varies from approx. 3mm in the cervical to about 9 mm in lumbar region. • The ratio between disk thickness and vertebral body height is greatest in the cervical and lumbar regions and least in the thoracic region. The greater the ratio, the greater the mobility, hence the disks in the cervical and lumbar regions contribute to the greater mobility in comparison with the thoracic region • The disk is composed of two parts; a central portion called the nucleus pulposus and a peripheral portion called the annulus fibrosus. • The composition of the nucleus and annulus are similar in that they both are composed of water, collagen, and proteoglycans (PGs). However the fluid and PG concentrations are highest in the nucleus and lowest in the outer annulus. Conversely collagen concentrations are highest in the outer annulus and lowest in the nucleus pulposus. • Maturation, aging and disease as well as normal and abnormal stresses on the disk may affect the distribution and relative proportions of type 1 and type 2 collagen.
- 13. Ligaments and Joint Capsules. • The ligamentous system of the vertebral column is extensive and exhibits considerable regional variability. There are 6 main ligaments associated with the intervertebral and zygapophyseal joints. I. Anterior longitudinal ligaments II. Posterior longitudinal ligaments III. ligamentum flavum IV. Interspinous V. Intertransverse VI. Supraspinous ligaments
- 14. Anterior and Posterior Longitudinal ligaments. • The anterior and posterior longitudinal ligaments are associated with the intervertebral joints. • The anterior longitudinal ligament runs along the anterior and lateral surfaces of the vertebral bodies from the sacrum to the second cervical vertebra. An extension the ligament from C2 to the occiput is called the anterior atlantoaxial ligament. • It has got two layers that are made up of thick bundles of collagen fibers. The fibers in the superficial layer are long and bridge several vertebrae, whereas the deep fibers are short and run between single pairs of vertebrae. • The ligament is well developed in the lordotic sections (cervical, lumbar) but has little substance in the region of thoracic kyphosis. The anterior longitudinal ligament increases in thickness and width from the lower thoracic to L5/S1. The tensile strength of the ligament is greatest at the high cervical, lower thoracic and lumbar regions. However when tested in axial tension, the ligament demonstrates its greatest tensile strength (675N) in the lumbar area. The ligament is compressed in flexion and stretched in extension and slack in the neutral position. The anterior longitudinal ligament is reported to be twice as strong as the posterior longitudinal ligament.
- 15. • The posterior longitudinal ligament runs within the vertebral canal along the posterior surfaces of the vertebral bodies from the second cervical vertebra to the sacrum. It consists of two layers, a superficial and a deep layer. • Superiorly the ligament continues to the occiput becoming the tectorial membrane at C2. in the lumbar region, the ligament narrows to a thin ribbon that continues into the sacral canal. The ligament provides little support for the intervertebral joints in the lumbar region. • The posterior longitudinal ligament’s resistance to axial tension in the lumbar area is only one sixth of that of the anterior longitudinal ligament ( 160N only). • It is stretched in flexion where maximal strain in the ligament occur s when it is slack in extension. However if the axis of motion moves posteriorly, as it does when the nucleus pulposus is destroyed either experimentally or by degenerative processes, the ligament may be stretched in extension.
- 16. Ligamentum Flavum • The ligamentum flavem is a thick, elastic ligament, which is located on the posterior surface of the vertebral canal. The fibers of the ligament run within the canal from the second cervical vertebra to the sacrum, connecting laminae of adjacent vertebrae. • In the lumbar region the ligament is composed of superficial and deep components. It attaches to adjacent laminae and contributes to the formation of the smooth dorsal wall of the spinal canal that abuts the dura. Most of the anterior surface of the lumbar laminae is covered by the ligamentum flavum. • It is the strongest in the lower thoracic and weakest in the midcervical region. Although the highest strain in this ligament occurs during flexion when the ligament is stretched, this ligament is under constant tension even when the spine is in a neutral position. The ligamentous tension creates a continuous compressive force on the disks, which causes the intradiskal pressure to remain high. The raised pressure in the disks makes the disks stiffer and thus more able to provide support for the spine in the neutral position.
- 17. Interspinous Ligaments • The interspinous ligaments vary from region to region. In the cervical and upper two thirds of the thoracic region, the ligaments connect and cover the margins of adjacent spinous processes. The parallel fibers of the ligaments run diagonally and fill up the space between the spinous processes. • In the lumbar region the ligaments are particularly well developed and attach to both the thoracolumbar fascia and the caudal fibers of the joint capsules. • The ligaments are slack in extension and stretched in forward flexion when they resist the separation of the spinous processes that accompanies flexion. The ligaments have a tensile strength of only 24 to 185 N and thus are potentially weaker in tensile strength than the anterior and posterior longitudinal ligaments and the ligamentum flavum.
- 18. Supraspinous Ligament • The supraspinous ligament is a strong cordlike structure that connects the tips of the spinous processes from the seventh cervical vertebra to L3 or L4. the fibers of the ligament become indistinct in the lumbar area where they merge with the thoracolumbar fascia and insertions of the lumbar muscles. • In the cervical region the ligament beccomes the ligamentum nuchae. The supraspinous ligament like the interspinous ligament is stretched in flexion and its fibers resist separation of the spinous processes during forward flexion. During hyperflexion the supraspinous and the interspinous are maximally stretched and are the first of the posterior ligaments to fail.
- 19. Intertransverse Ligaments • The ligaments pass between the transverse processes and attach to the deep muscles of the back. In the cervical region only a few fivers of the ligaments are found. • The membranous fibers of the ligament form part of the thoracoluumbar fascia. • The ligaments are alternatively stretched and compressed during lateral bending. The ligaments on the right side are stretched and offer resistance during lateral bending to the left while the ligaments on the left side are slack and compressed during this motion and vice versa.
- 20. Zygapophyseal Joint Capsule • The zygapophyseal joint capsules assist the ligaments in providing limitation to motion and stability for the spine. The capsule s are strongest in the thoracolumbar region and at he cervicothoracic junction sites where the spinal configuration changes from a kyphotic to lordotic curve and from a lordotic to kyphotic curve, respectively. • The joint capsules, like the supraspinous and interspinous ligaments, are vulnerable to hyperflexion, especially in the lumbar region. It provide more restraint to forward flexion than any of the posterior ligaments because they fail after the supraspinous and interspinous ligaments when the spine is hyperflexed.
- 22. Functions of Spine. • Stability: • The stiffness of the vertebral column is the column’s ability to resist an applied load. Stiffness can be represented graphically by the slope of the stress-strain curve. The steeper the slope of the curve, the stiffer the structure. • By applying a specified load to a motion segment (two adjacent vertebrae and the intervening soft tissues) stiffness of that particular segment can be determined. • The neutral zone is the ROM through which the spine can be displaced from a neutral position to the point at which elastic deformation begins when a small load is applied. In a stress-strain curve the neutral zone would be represented by the toe region of the curve. • Punjabi has suggested that the existence of a large neutral zone indicates instability. Instability of the vertebral column can be considered as a lack of stiffness and an unstable structure is one that is not in an optimal state of equilibrium. • The spine is subjected to axial compression, tension, bending, torsion and shear stress not only during normal functional activities but also at rest which depend upon the type, duration and rate of loading; the person’s age and posture; the condition and properties of the various elements.
- 23. Axial Compression. • Axial compression (force acting through the long axis at an 90 degree) occurs due to the force of gravity, ground reaction forces and forces produced by the ligaments and muscular contractions. Most compressive force is resested by the disks and vertebral bodies, but the arches and zygapophyseal joints share some of the load in certain postures and during specific motions. The compressive load is transmitted from the superior end plate to the inferior end plate through the trabecular bone of the vertebral body and the cortical shell. • The cancellous body contributes 25%-55% of the strengthof a lumbar vertebra under the age of 40yrs and the cortical bone carries the remainder. • Depending on the posture and region of the spine, the zygapophyseal joints carry from 0%-33% of the compression load. The spinous processes also may share some of the load when the spine is in hyperextension. • The nucleus pulposus acts as a ball of fluid that can be deformed by a compression force. The pressure created in the nucleus actually is greater than the force of the applied load.
- 24. When a weight is applied to the nucleus pulposus from above, the nucleus loses height as it exhibits a swelling pressure and tries to expand outward toward the annulus and the end plates. As the nucleus attempts to distribute the pressure in all directions, stress is created in the annulus and central compressive loading occurs on the vertebral end plates. • The forces of the nucleus on the annulus and the annulus on the nucleus form an interaction pair which provide sufficient resistance to the swelling pressure in the nucleus to reach an maintain a state of equilibrium. • The pressure exerted on the end plates is transmitted to the superior and inferior vertebral bodies. The annulus fibrosus is under tensile stress and thus is able to better resist he compressive load. The disks and trabecular bone are able to undergo a greater amount of deformation without failure than the cartilaginous end plates or cortical bone when subjected to axial compression. The end plates are able to undergo the least deformation and therefore will be the first to fail/ failure under high compressive loading. The disks will be the last to fail. • The disks are subjected to a constant load by forces that are not large enough to cause permanent damage, the disks exhibit creep. The recovery of fluid that returns the disk to its original state explains why a person getting up from bed is taller in the morning than in the evening and why an astronaut returning from weight weightlessness of space is taller on his return than on his departure. • Running is a form of dynamic loading that decreases disk height more rapidly than static loading. The loss of height that occurs as people grow older is due to the fact that the nucleus loses a large proportion of its fluid-imbibing capacity with aging.
- 25. Bending • Bending causes both compression and tension on the structures of the spine. In forward flexion the anterior structures are subjected to compression; the posterior structures are subjected to tension. The resistance offered to the tensile forces by collagen fibers in the posterior outer annulus fibrosus, zygapophyseal joint capsules, and posterior ligaments help to limit extremes of motion and hence provide stability in flexion. • The resulting deformation of supporting structures such as ligaments, joint capsules, and intervertebral disks leads to an increase in the ROM beyond normal limits and places the vertebral structures at risk of injury. • In extension the posterior structures generally are either unloaded or subjected to compression, whereas the anterior structures are subjected to tension. Resistance to extension is provided by the anterior outer fibers of the annulus vibrosus, zygapophyseal joint capsules, passive tension in the anterior longitudinal ligament and by contact of the spinous processes. • In lateral bending, the ipsilateral side of the disk is compressed; that is, in right lateral bending the right side of the disk is compressed while the outer fibers of the left side of the disk are stretched so the contralateral fibers and ligaments help to provide stability.
- 26. Torsion • Torsional forces are created during axial rotation that occurs as a part of the coupled motions that take place in the spine. The torsional stiffness in flexion and lateral bending of the upper thoracic region from T1 to T6 is similar in stiffness, but torsional stiffness increases from T7/T8 to L3/L4. • Tortional stiffness is provided by the outer layers of both the vertebral bodies and intervertebral disks and by the orientation of the facets. • The outer shell of cortical bone reinforces the trabecular bone and provides resistance to torsion. • When the disk is subjected to torsion, one half of the annulus fibers resist clockwise rotations, whereas fibers oriented in the opposite direction resist counter clockwise rotations. It has been suggested that the annulus fibrosus may be the most effective structure in the lumbar region for resisting torsion. • The risk of rupture of the disk fibers is increased when torsion, heavy axial compression and bending are combined.
- 27. Shear • Shear forces act on the mid plane of the disk and tend to cause each vertebra to undergo translation (move anteriorly, posteriorly or from side to side in relation to the inferior vertebra) • In the lumbar spine the zygapophyseal joints resist some of the shear force and the disks resist the remainder. When the load is sustained, the disks exhibit creep and the zygapophyseal joints may have to resist all of the shear force.
- 28. Mobility • Motions at the intervertebral and zygapophyseal joints are interdependent. The amount of motion available is determined primarily by the orientation of the facets. The motion that occurs between the vertebral bodies at the intervertebral joints is similar to what occurs when a rubbing ball is placed between two blocks of wood. The blocks ma be tilted or rotated in any direction and may glide if the ball rolls. • The motions of flexion and extension occur as a result of the tilting and gliding of a superior vertebra over the inferior vertebra. • The nucleus pulposus acts like a pivot but unlike a ball is able to underfo greater distortion because it behaves as a fluid. • The magnitude of motion created by the ratio of disk height to width, a gliding motion occurs at he zygapophyseal joints as the vertebral body tilts over the disk at the intervertebral joint. • If the superior and inferior zygapophyseal facet surfaces of three adjacent vertebrae lie in the sagittal plane, the motions of flexion and extension are facilitated. If the zygapophyseal facet surfaces are placed in the frontal plane the predominant motion that is allowed is that of later flexion.
- 29. Flexion • In vertebral flexion the anterior tilting and gliding of the superior vertebra causes a widening of the intervertebral foramen and a separation of the spinous processes. • The amount of tilting is partly dependent on the size of the disks, tensionin the supraspinous and interspinous ligaments resists separation of the spinous processes and thus limits tje extent of flexion. Passive tension tn the zygaapophyseal joint capsules, ligamentum flavum, posterior longitudinal ligament, posterior annulus, and the back extensors also imposes controls on excessive flexion. Tension in the posterior ligaments can be produced by contractions of the hip extensors pulling downward on the pelvis when a person is in the standing position. • Tension in the thoracolumbar fascia produced by contractions of the transversus abdominis also can limit flexion by the pull of the fascia on the spinous processes in the lumbar area. • The disks influence flexion because the anterior portion of the annulus fibrosus is compressed and bulges anteriorly during flexion while the posterior portion is stretched and resists separation of the vertebral bodies.
- 30. Extension • In extension, the intervertebral foramen is narrowed and the spinous processes move closer together. The amoutnt of motion available in extension, in addition to being limited by the size of the disks, is limited by bony contact of the spinous processes, passive tension in the zygapophyseal joint capsules, anterior fibers of the annulus, anterior trunk muscles, and the anterior longitudinal ligament. • There are many more ligaments that limit flexion than there are ligaments that limit extension. • The only ligament that limits extension is the anterior longitudinal ligament. The numerous checks to flexion follow the pattern of finding ligamentous checks to motion where bony limits are minimal. • Few ligamentous checks to extension are necessary given the presence of numerous bony checks.
- 31. Lateral Flexion • In lateral flexion, the superior vertebra tilts, rotates and translates over the adjacent vertebra below. The annulus fibrosus is compressed on the concavity of the curve and stretched on the convexity of the curve. Passive tension in the annulus fivers, intertransverse ligaments and anterior and posterior trunk muscles on the convexity of the curve limit lateral flexion, the rotation that accompanies lateral flexion differs slightly from region to region because of the orientation of the facets. • All intervertebral and zygapophyseal joint motion that occurs between the vertebrae from L5 to S1 adheres to the general description that have been presented. Regional variations in the structure, function and musculature of the column are different in different region.
- 32. Regional Variations in Vertebral Str. Part Cervical Vert. Thoracic Vert. Lumbar Vert. Body The body is small with a transverse diameter greater than anterior posterior diameter. Anterior surface of the body is convex; posterior surface is flat. The superior surface of the body is saddle shaped due to the presence of uncinate processes on the lateral aspects of the superior surfaces. The transverse and anterior posterior diameters of the bodies are equal. Anterior height is greater than posterior. Two demifacets for articulation with the ribs are located on the postero lateral corners of the vertebral plateaus. The body is massive a transverse diameter greater than the anterior posterior diameter and height. Pedicles Project posterolaterally. Variable in shape and orientation Short and thick Laminae Project posteromedially and are thin and slightly curved. Short, thick and broad Short and broad
- 33. Spinous processes Short, slender and extend horizantally.have bifid tips. T1-T10 slope inferiorly T11 and T12 have a triangular shape. Broad, thick and extend horizantally. Vertebral foramen Large and roughly triangular. Small and circular Triangular. It is larger than the thoracic but smaller than the cervical. Superior zygapophyse al facets Face superiorly and medeally. Thin and flat and face posteriorly, superiorly and laterally. Vertical and concave and face posteromedially. Support mamillary processes on posterior borders. Inferior zygapophyse al facets Face anteriorly and laterally. Face anteriorly, superiorly and medially. Vertical, convex and face anterolaterally. Transverse processes Prossess foramen for vertebral artery, vein and venous plexus. Also have agutter for spinal nerve. Processes are large with thickened ends. Possess paired oval facets for articulation with the ribs. Show a caudal decrease in Processes are long, slender and extend horizontally. They support accessory processes o the posterior inferior
- 34. Muscles of the Spine • Flexors: • Muscles that flex the trunk are located anteriorly and laterally with attachments on the ribs, sternum and pelvis these muscles act indirectly on the vertebral column by exerting a pull on the adjacent structures. Contractions of the flexor muscles cause compression forces on the vertebral column. • When the pelvis and ribs are free to move, a shortening contraction of the flexors will pull these structures closer together and as a consequence flex the total spine as in a sit up. • If the ribs are fixed, a shortening contraction of the rectus abdominis muscle will exert an upward pull on the anterior pelvis. The resulting posterior rotation of the pelvis in the sagittal plane (posterior pelvic tilt) will flex the contiguous lumbar spine. • The internal and external oblique abdominal muscles turn and twist the lumbar spine into axial rotation. • The psoas major muscle has been described as a flexor, as a stabilizer and as an extensor of the lumbar spine.
- 35. Rotators and Lateral flexors • Rotation of the trunk is usually coupled with some degree of lateral flexion. Anterior muscles that produce rotation and lateral flexion are the external and internal oblique abdominals. • Rotation of the trunk to the left requires a simultaneous contraction of the right external oblique and the left internal oblique and vice versa. • Rotation and lateral flexion to the same side are a function of the iliocostalis, longissimus, spinalis muscles, quadratus lumborum and serratus posterior superior. • Muscles that produce rotation to the opposite side are the semispinalis thoracis, multifidus, rotatores and intertransversarii thoracis. • The lateral flexors of the trunk are the quadratus lumborum and the iliopsoas.
- 36. Extensors • Muscles that extend the vertebral column are located posteriorly. The sacrospinalis muscles (erector spinae), consist of three divisions. This group of muscles extends from the sacrum to the occipital portion of the skull, attaching to the transverse and spinous processes of all vertebrae and the angles of the ribs by various divisions. • Lateral division- attaches to the ribs is called the iliocostalis group and consists of the iliocostalis cervicis, thoracis and lumborum. • Medial division- attaches to the spinous processes and is called the spinalis group, which includes the spinalis cervicis, capitis and thoracis. • Intermediate division- attaches to the transverse processes is called the longissimus, which includes the longissimus capitus, cervicis and thoracis.
- 38. Thank- You